SciBase Journals
SciBase Addiction & Recovery
- Article Type: Research Article
- Volume 1, Issue 1
- Received: Jul 09, 2024
- Accepted: Sep 02, 2024
- Published Online: Sep 09, 2024
Simultaneously Ventral Hernia Repair with Abdominoplasty: A Feasible Approach
Gaetano Vetrone1; Luca Negosanti1,2*; Rossella Sgarzani3; Romano Linguerri1; Michele Masetti1
1General Surgery, S. Maria Della Scaletta Hospital, Imola, Italy.
2Montecatone Rehabilitation Institute, Imola, Italy.
3DIMES, University of Bologna, Italy.
*Corresponding Author: Luca Negosanti
CGeneral Surgery, S. Maria Della Scaletta Hospital, Imola,
Italy.
Email: luca.negosanti@montecatone.com
Abstract
Purpose: Repair of ventral hernias still represents a challenge and, in some cases, patients present a concomitant abdominal wall laxity and an excess of skin and subcutaneous fat. The association of ventral hernia repair and abdominoplasty remains controversial. The aim of this study is to present our experience in the association of ventral hernia repair and abdominoplasty, both in open surgery and in laparoscopy.
Methods: In this retrospective study, 12 patients were operated with simultaneously hernia repair and abdominoplasty, between January 2018 and January 2023. Patients were followed to monitor incidence of complications and hernia recurrence. There were 4 hernias treated laparoscopically and 8 hernias treated laparotomically. Mean defect size was 8.6 cm in width and 9.8 cm in length. There were 4 giant midline ventral hernia. Mean BMI was 31 kg/m2 (range 21-44) and the mean operative time was 165 minutes (range 120-224 minutes). The mean postoperative length of hospital stay was 8.7 days, ranging from 4 to 31 days.
Results: No mortality or major complications encountered. There were 2 (16%) wound complications occurred in obese patients: 1 subcutaneous seroma treated with Vacuum Assisted Closure® (VAC) therapy and 1 subcutaneous hematoma, that was evacuated. No patients suffered wound infection. After a mean follow-up of 812 days, 1 (8,6%) recurrence was registered.
Conclusion: We believe that the simultaneous approach, consisting in ventral hernia repair combined to abdominoplasty, is an effective and safe technique for reconstruction of patients with abdominal hernia and simultaneously excess of skin and subcutaneous fat.
Keywords: Abdominoplasty; Hernia; Laparocele; Abdominal wall reconstruction; Laparoscopy.
Citation: Vetrone G, Negosanti L, Sgarzani R, Linguerri R, Masetti M. Simultaneously Ventral Hernia Repair with Abdominoplasty: A Feasible Approach. SciBase J Addict Recovery. 2024; 1(1): 1002.
Introduction
Reconstruction of abdominal wall defects could be a challenging problem. Patients with large midline ventral hernias usually present abdominal wall laxity and external deformity due to an excess of skin and subcutaneous fat [1]. There are different options to repair of abdominal wall defects and the choice is principally based on the size of the defect. General surgeons usually avoid adding abdominoplasty to the hernia repair, thinking that this secondary procedure led to higher morbidity and longer surgical time. This belief originates from the lack of adequate evidence in literature and, also, because there are few evidence-based guidelines concerning preoperative decision making and risk counselling when abdominoplasty is combined to hernia repair. However, some surgeons give their patients a complete solution to their problems, performing simultaneous hernioplasty and abdominoplasty [2-7]. In this paper we present our recent experience in the combination of ventral hernia repair with abdominoplasty, to repair abdominal wall defect, provide a better aesthetic outcome and avoid further surgery, analyzing the incidence of short-and long-term complications of the combined technique.
Materials and methods
In this retrospective study, 12 patients were operated with simultaneously hernia repair and abdominoplasty, between January 2018 and January 2023. These patients had abdominal wall hernias or severe rectus abdominis diastasis and associated skin laxity and excess of subcutaneous fat. Hernia repair was performed with laparoscopic IPOM technique (using a Ventralight mesh) or with a laparotomic approach with intraperitoneal prosthesis as previously described [8]. The abdominoplasty was performed by a plastic surgeon. If we choose a laparoscopic approach to repair the wall defect, you to make it first. If the laparotomic approach was planned, the plastic surgeon starts surgery.
The abdominoplasty was performed as described here. Through a suprapubic incision, the abdominal flap is dissected from the muscle fascia and the navel is isolated. The dissection is performed to reach the costal arch and the xyphoid, in a bell shape, larger in the central portion and thinner laterally, to preserve the vascularization of the abdominal flap. Then, the excess of skin and subcutaneous tissue is resected to obtain a tension free suture. In case of laparotomic repair of the hernia, the muscle is exposed, and hernia is repaired [12]. Sutures are then made, and navel is repositioned trough a triangular incision of the abdominal flap. A contenitive dressing is performed. Antibiotics are administered for 3 days after surgery. Drains are removed on the hospital discharge (usually after 5-7 days). Patients are discharged wearing abdominal binder since immediate postoperative till 2 months later, then they are clinically evaluated at 1, 6 and 12 months after surgery. Evaluation parameters are operation time, length of hospital stay, early morbidity and recurrence rate. The recurrence rate is defined at 6 and 12 months and the aesthetic outcome is evaluated by patient and surgeon satisfaction rate at the last postoperative evaluation. Informed consent and consent to publish is collected by the authors prior to the surgery.
Results
The study included 12 patients (11 female). The characteristics of the patients are summarized in Table 1. Age ranged from 34 to 74 years, and BMI ranged between 21 and 44 kg/m2 with a mean of 31 kg/m2. The mean operative time was 165 minutes (range 120-224 minutes). The mean postoperative length of hospital stay was 8.7 days ranging from 4 to 31 days. There are 7 midline incisional hernia, 1 suprapubic hernia, 1 left lateral trocar site hernia, 2 primitive umbilical hernia, 1 large diastasis of rectus abdominis muscles (7 cm in width). In 4 (30%) patients the hernia was repaired with a laparoscopic approach (figures 1-3), while, in the other 8 (70%), the hernia was repaired using an open technique. There were 2 (16%) wound complications occurred in obese patients: 1 seroma treated with Vacuum Assisted Closure® (VAC) therapy and 1 hematoma, that was evacuated. After a mean follow-up of 812 days (range 84-1706), 1 (8 %) recurrence was detected.
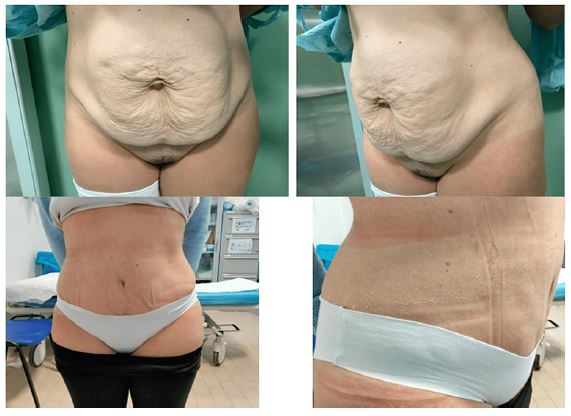


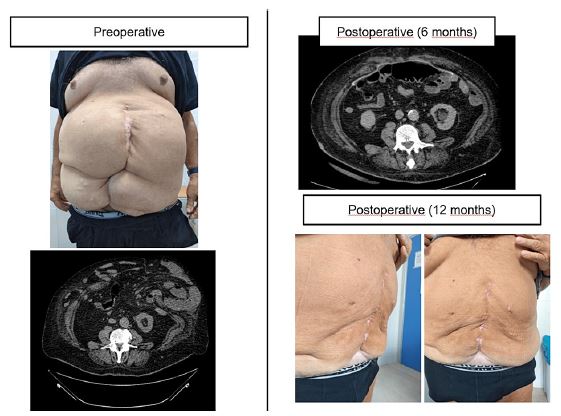
Table 1: Patient’s characteristics.
| Age (years) | 54(34-74) |
| Sex Female | 11(91%) |
| Diabete | 0 |
| BMI | 31(21-44) |
| Timing (min) | 165(120-224) |
| Hospital stay (days) | 8.7(4-31) |
| Hernia type |
Midline incisional 7 Suprapubic incisional 1 Umbilical hernia 2 Lateral trocar site 1 Diastasis of recti 1 |
| Hernia size Width (cm) Lenght (cm) | 8.6(3-18) 9.8(3-20) |
| Laparoscopic IPOM | 4(30%) |
| IPOW (“OPEN-IPOM”) | 8(70%) |
| Complications | Hematoma 2(16%) |
| Hernia recurrence | 1(8.6%) |
| Follow up (days) | 812(84-1706) |
Discussion
The repair of ventral hernias still represents a challenge for surgeons. The current opinion is that surgery must be tailored according to hernia characteristics and concomitant conditions. Sometimes, ventral hernias coexist with rectus abdominis diastasis, myofascial weakness, skin laxity and an excess of subcutaneous fat with abdominal deformity. All these defects can be solved in a comprehensive operation to avoid other surgery without adding more morbidities [9]. For long time, surgeons avoid adding abdominal remodeling procedures to hernia repair, thinking that, these added procedures, can led to higher morbidity and longer surgical time [5-7]. We believe that a multidisciplinary approach is necessary in this type of simultaneous surgery: general surgeon for hernia repair and plastic surgeon for abdominoplasty, and a preoperative planning is fundamental to define the correct procedure and to reduce risk of complications. In this study, we described a simultaneous approach of ventral hernia repair and abdominoplasty. Meanwhile, we have monitored the incidence of short- and long- term complications. In this study we performed laparoscopic approach for small defects, and this is particularly interesting. The association of laparoscopic repair with abdominoplasty allows to maintain intact the healthy wall beyond the defect and the prosthesis is positioned in a “protected” seat under the superficial planes. The ideal case is a symptomatic umbilical hernia, where the defect is small, and the results of laparoscopic correction are optimal. Laparoscopic surgery is known to have dramatically reduced wound infections [10]: this is a revolutionary result in hernia surgery, and it is extremely useful if we associate abdominoplasty. The indication for laparoscopic surgery versus open surgery is mainly given by the transverse diameter of the defect. Generally, defects with a diameter of less than 6-7 cm are performed laparoscopically, otherwise we propose open surgery. We have recently developed a technique for the treatment of large incisional hernias using an intraperitoneal prosthesis with without performing the muscle dissections [8]. This approach allows to reduce the surgical site complications related to muscle dissections. In all cases of parietal defects we use a mesh, we do not perform direct sutures of hernias, even small ones. Also, this approach is particularly helpful when an abdominoplasty is associated which represents itself an additional source of risk of hematomas and seromas. Indeed, considering the complexity of the surgery, the wound complications were very low (2 hematomas in obese patients). Shermack [11] found that the complications encountered when combining abdominoplasty with herniorraphy are the same as those encountered when the procedures are performed separately, with the most frequent including wound complications (20%), and seroma (12.5%). Finally, we recorded only 1 recurrence in the follow-up period in a very large midline hernia in an obese patient (Figure 4).
Conclusion
This simultaneous approach is an effective method to reconstruct ventral hernias defects and provide a more aesthetic postoperative appearance of the abdomen in appropriately selected patients. The combined procedure is safe and effective, both for small defects and in case of large ventral hernia. This procedure allows to obtain a good result in a single surgery, avoiding further interventions and no increasing the risk of complications. The multidisciplinary approach is fundamental in these cases. General and plastic surgeon must evaluate each case together to define the correct procedure and to obtain optimal results. Further studies must be necessary to confirm the reported results.
Declarations
Statements: The authors declare that no funds, grants, or other support were received during the preparation of this manuscript. The authors have no relevant financial or non-financial interests to disclose.
Ethics approval: This is an observational study. Our Ethics Committee has confirmed that no ethical approval is required.
Consent to participate: As retrospective study the consent is not required by our Ethical Committee.
Consent to publish: The authors affirm that human research participants provided informed consent for publication of the images.
Financial disclosures: None of the authors has a financial interest in any of the products, devices, or drugs mentioned in this manuscript.
References
- Switzer NJ, Dykstra MA, Gill RS, et al. Endoscopic versus open component separation: Systematic review and meta-analysis. Surg Endosc. 2015; 29: 787-795. 10.1007/s00464-014-3741-1.
- Ramirez OM. Abdominoplasty and abdominal wall rehabilitation: A comprehensive approach. Plastic Reconstruct Surg J. 2000; 105: 425-435. 10.1097/00006534-200001000-00069.
- Heller L, McNichols CH, Ramirez OM: Component separations. Semin Plast Surg. 2012; 26: 25-28. 10.1055/s-0032-1302462.
- Moreno-Egea A, Campillo-Soto A, Morales-Cuenca G. Does abdominoplasty add morbidity to incisional hernia repair? A randomized controlled. Trial Surg Innov. 2016; 23: 474-480. 10.1177/1553350616646480.
- Koolen PG, Ibrahim AM, Kim K, et al. Patient selection optimization following combined abdominal procedures: analysis of 4925 patients undergoing panniculectomy/ abdominoplasty with or without concurrent hernia repair. Plast Reconstr Surg. 2014; 134: 539 e-550 e. 10.1097/PRS.0000000000000519.
- Mazzocchi M, Dessy LA, Ranno R, Carlesimo B, Rubino C. Component separation technique and panniculectomy for repair of incisional hernia. Am J Surg. 2011; 201: 776-783. 10.1016/j.amjsurg.2010.04.013.
- McKnight CL, Fowler JL, Cobb WS, Smith DE, Carbonell AM. Concomitant sublay mesh repair of umbilical hernia and abdominoplasty. Can J Plast Surg. 2012; 20: 258-260. 10.1177/229255031202000413.
- Vetrone G, Linguerri R, Negosanti L, Masetti M. Intraperitoneal mesh open repair without dissection technique for large ventral hernia repair: an alternative to component separation technique. Minerva Surg. 2023. 8:10.23736/S2724-5691.23.09849-0.
- Erfan MA, Nasser S, Wardany IE, et al. Ventral hernia repair in conjunction with lipoabdominoplasty in overweight patients: A comprehensive approach. Int Wound J. 2023; 1-8. 10.1111/iwj.14011.
- Linea guida Trattamento laparoscopico del laparocele ed ernie ventrali - Linee guida italiane (SICE). Linea guida pubblicata nel Sistema Nazionale Linee Guida Roma, 28 febbraio. 2022. https://www.iss.it/-/snlg-trattamento-laparoscopico-del-laparocele.
- Shermak MA. Hernia Repair and Abdominoplasty in Gastric Bypass Patients. PRS. 2006; 117: 1145-1150. 10.1097/01.prs.0000204587.10550.21.