SciBase Journals
SciBase Cardiology
ISSN 2996-4547
- Article Type: Research Article
- Volume 2, Issue 2
- Received: Aug 23, 2024
- Accepted: Oct 02, 2024
- Published Online: Oct 09, 2024
Transforming Marfan Syndrome Diagnosis with AI and Federated Learning
Venkatesh Upadrista1*; Stefan Schulze2
1Department of Computing, Glasgow Caledonian University, Glasgow G4 0BA, Scotland.
2Chief Executive Officer, Vifor Pharma, Scotland.
*Corresponding Author: Venkatesh Upadrista
Department of Computing, Glasgow Caledonian University,
Glasgow G4 0BA, Scotland.
Tel: +44-0-7424991399;
Email: vupadr200@caledonian.ac.uk
Abstract
Marfan Syndrome is a genetic disorder affecting connective tissue, leading to severe cardiovascular, skeletal, and ocular complications. Early detection is essential to prevent critical outcomes such as aortic aneurysms and dissections. However, traditional diagnostic methods, including advanced imaging and genetic testing, are often expensive and invasive. This study proposes a two-stage diagnostic model combining non-invasive physical evaluations and advanced diagnostic tests to improve resource utilization and enhance early detection.
The first stage utilizes a Convolutional Neural Network (CNN) to detect key physical signs of Marfan Syndrome, such as elongated limbs and scoliosis, using clinical imaging data. For patients flagged as high-risk, the second stage employs advanced diagnostic techniques, including echocardiograms, MRI, CT scans, and genetic testing, to confirm the diagnosis. Data from 12,826 patient records, provided by The Marfan Foundation, were used, including echocardiograms, MRI/CT scans, genetic data, and follow-up information. The CNN model achieved an accuracy between 91% and 94%, demonstrating its effectiveness in identifying physical indicators. The YOLOv8 object detection models, used in the second stage with a federated learning approach, achieved a mean Average Precision (mAP) of 0.994 and 0.995. These results highlight the potential of AI-driven federated learning models to enhance the accuracy and efficiency of Marfan Syndrome diagnosis, reducing unnecessary testing and improving patient outcomes. Future work will focus on expanding the dataset and integrating data from multiple institutions to further improve the model’s generalizability.
Keywords: Machine learning; Marfan syndrome detection; Federated learning; Convolutional neural networks (CNN); YOLOv8 object detection models; Non-invasive diagnostic methods; AI-driven genetic disorder diagnosis.
Citation: Upadrista V, Schulze S. Transforming Marfan Syndrome Diagnosis with AI and Federated Learning. SciBase Cardiol. 2024; 2(2): 1012.
Introduction
Marfan Syndrome is a genetic disorder affecting the connective tissue, leading to complications in various organs, particularly the cardiovascular system. The most dangerous complications, such as aortic aneurysms and dissections, often develop without warning and can be life-threatening before they are detected. Early diagnosis is critical to prevent these catastrophic outcomes, but the condition is notoriously difficult to diagnose due to the variability of its symptoms and the subtlety of earlystage indicators.
Common physical signs such as elongated limbs, scoliosis, and chest deformities may go unnoticed or be mistaken for normal variations in body structure, further delaying diagnosis. Traditional diagnostic methods, such as MRI and genetic testing, are expensive and invasive, making them impractical for widespread screening. As a result, many cases of Marfan Syndrome are not detected until serious complications arise, missing critical opportunities for early intervention and management.
Our literature review identified key gaps in the diagnosis and management of Marfan Syndrome, including the need for improved diagnostics, psychological support, enhanced treatment, and long-term monitoring. Studies [1-3] highlighted reduced physical fitness, the role of the nitric oxide pathway in aortic disease, and the impact of chronic pain on quality of life. Research [4-6] emphasized the challenges of diagnosing Marfan Syndrome due to phenotypic variability, while studies identified potential therapeutic targets like the C3a/C3aR pathway and stressed the importance of continuous imaging post-surgery. Studies [7-10] revealed discrepancies in monitoring techniques, challenges in low-resource settings, underdiagnosis due to limited genetic testing, and the link between sleep apnea and cardiovascular mortality in Marfan Syndrome patients.
Despite the recognized importance of early diagnosis, there are currently no widely adopted predictive models for Marfan Syndrome. This is a significant gap in the diagnosis of genetic disorders, particularly for population-wide screening. To address this, our AI-driven model offers a scalable and accessible solution that can be integrated into various healthcare environments, facilitating early intervention, and improving patient outcomes.
Our model features a two-phase approach to enhance diagnostic efficiency while conserving healthcare resources. The first phase uses non-invasive methods, such as a Convolutional Neural Network (CNN) trained to detect physical signs of Marfan Syndrome, enabling early identification without expensive or invasive procedures. The second phase involves specialized diagnostic tools like MRI, CT scans, and genetic testing for high-risk patients. This model uses federated learning to collaboratively improve diagnostic accuracy while maintaining patient data privacy. Through this advanced AI-driven approach, our model can transform the detection and management of Marfan Syndrome, leading to earlier interventions and better patient care.
Evaluation of our model showed strong results in both screening and diagnostic stages, with accuracy, precision, and recall rates exceeding 90%. This demonstrates the model’s reliability as a tool for early detection and management of Marfan Syndrome, ultimately contributing to improved outcomes and reduced mortality for patients with this complex genetic disorder.
Literature review
As part of [1], authors explored physical fitness in children with Marfan and Loeys-Dietz syndromes. They identified significant reductions in physical fitness and strong associations with self-reported fatigue. The paper addressed challenges in improving physical activity and participation, emphasizing tailored exercise programs as a solution to enhance fitness and reduce fatigue in affected children.
A very important subject has been covered in [2], where authors explored the role of the nitric oxide (NO)-sGC-PRKG signaling pathway in Marfan Syndrome (MFS) aortopathy. The study identified overactivation of this pathway as a key driver of aortic disease in MFS, providing potential therapeutic targets. Challenges addressed include understanding the molecular mechanisms underlying aortic dilation and developing new interventions.
As part of [3], authors explored the quality of life in young patients with acute type A aortic dissection (AAAD) in China, comparing those with and without Marfan syndrome (MFS). Challenges such as persistent chronic pain and anxiety were identified, with MFS patients experiencing significantly lower quality of life post-surgery. The study emphasized the need for targeted psychological and pain management interventions.
Authors in [4], investigated the genotype-phenotype relationship in children with Marfan Syndrome (MFS) in Southeastern Anatolia. The paper addressed the challenges in diagnosing MFS in children due to phenotypic variability and age-related symptom onset. The study emphasized the importance of long-term monitoring and bioinformatic reanalysis for an accurate genotype-phenotype correlation.
As part of [5], authors investigated the role of the complement system in Marfan syndrome (MFS)-associated Thoracic Aortic Aneurysm (TAA). They found that complement activation, particularly the C3a/C3aR pathway, contributed to aneurysm development in MFS. The study addressed challenges by demonstrating that inhibiting this pathway with a C3aR antagonist reduced inflammation and aortic dilation in MFS mice, highlighting a potential therapeutic target.
A very important subject was covered in [6] which analyzed long-term outcomes in Marfan syndrome patients who underwent aortic root replacement. The research found that distal aortic dilation progressed more rapidly in these patients compared to those without surgery, highlighting the need for continuous monitoring. The study addressed challenges in post-surgical aortic complications and emphasized lifelong imaging follow-up.
Authors in [7] compared echocardiography (TTE) and Computed Tomography (CT) in the initial assessment and 2-year follow-up for monitoring Marfan syndrome and related disorders. The study revealed significant discrepancies in aortic measurements between TTE and CT, with CT providing more accurate results. The challenges addressed include improving monitoring techniques to prevent life-threatening aortic complications.
As part of [8] authors examined the challenges in diagnosing and surgically correcting Marfan syndrome-associated aortic disease in a middle-income country. The study identified delayed diagnosis, limited resources, and emergent surgeries as significant challenges, impacting reintervention rates. The authors emphasized the importance of prompt diagnosis, surveillance programs, and educational initiatives to improve outcomes in resource-constrained settings.
As part of a population-based study in [9] authors revealed an underdiagnosis of Marfan Syndrome (MFS) by identifying pathogenic FBN1 variants. They found that clinical diagnoses alone underestimated MFS prevalence, which was revised from 1 in 10,000 to 1 in 6,600. The study addressed challenges in diagnosing mild cases of MFS and highlighted the importance of combining genetic and clinical data.
A very important subject was covered in [10] where authors found that sleep apnea predicts cardiovascular death in Marfan Syndrome (MFS) patients. The study addressed challenges in managing MFS by identifying sleep apnea as an independent risk factor for cardiovascular mortality. The paper emphasized the need for routine sleep apnea screening in MFS patients to improve personalized treatment and prevent cardiovascular deaths.
Methodology
Our methodology is split into two distinct stages: Basic Physical Evaluation and Specialized Diagnostic Tests. Each stage is tailored to progressively refine the diagnostic process, minimizing unnecessary advanced testing and optimizing the use of healthcare resources.
Basic physical evaluation
The first diagnostic stage involves non-invasive basic physical tests that can be performed at home or during regular check-ups. These tests focus on identifying key clinical indicators of Marfan Syndrome. To support this, we developed a Convolutional Neural Network (CNN) model capable of analyzing simple body images to identify potential signs of Marfan Syndrome. By focusing on visible physical symptoms, this stage allows for early screening, reducing the need for advanced and invasive tests for every patient.
Family history integration: Marfan Syndrome is an inherited condition, and understanding a patient’s family history is crucial for risk assessment. We integrate family history data with body image analysis to determine the likelihood of the syndrome.
We developed a user interface (Figure 1) where patients can upload their pictures, such as the one depicted in Figure 2. Once submitted, the CNN model predicts the occurrence of the syndrome.


CNN model design and training
CNNs are well-suited for medical image analysis due to their ability to learn and recognize complex patterns. We evaluated several CNN architectures, including LeNet, AlexNet, and VGG-16. VGG-16 was selected due to its superior performance, leveraging deeper layers and smaller convolutional kernels to improve detection accuracy.
Key clinical indicators
The model was trained to identify several critical physical symptoms associated with Marfan Syndrome:
Long Limbs (Arachnodactyly): The model detects limb length disproportion, a characteristic symptom of Marfan Syndrome.
Scoliosis (Curved Spine): The model analyzes spinal curvature from side and back images, detecting abnormal curvatures indicative of scoliosis.
Chest Deformities (Pectus Excavatum or Pectus Carinatum): The model identifies abnormal chest shapes and contours, including inward and outward deformities.
Lens dislocation: The model detects signs of ectopia lentis, an ocular manifestation of Marfan Syndrome.
Aortic Abnormalities: Initial signs of aortic dilation or aneurysm are flagged for further examination.
Datasets
Limited datasets are available for detecting Marfan Syndrome. We used the Skeletal Dataset from OrthoBullets [11] , which includes measurements and radiographs indicating skeletal abnormalities, such as long limbs, scoliosis, and protrusio acetabuli. Imaging data like X-rays and MRI scans provide crucial insights into these orthopedic manifestations.
Specialized diagnostic tests
For patients flagged as potentially positive during the Basic Physical Evaluation, we proceed with specialized diagnostic tests to confirm the diagnosis. This stage involves advanced imaging and genetic testing to accurately assess the severity of the condition and identify specific abnormalities associated with Marfan Syndrome. To enhance the accuracy and robustness of these specialized diagnostics, we utilized federated learning.
Federated learning offers significant advantages in this context. By allowing multiple medical institutions or nodes to collaboratively train diagnostic models without sharing sensitive patient data, federated learning ensures data privacy and security. Each node can retain its local data, such as imaging and genetic information, while contributing to a more comprehensive and diverse model through the aggregation of model updates. This results in a global model that benefits from a broader range of patient data, leading to improved detection accuracy and better generalization across different populations. Moreover, federated learning reduces the risk of bias that can occur when a model is trained on a single dataset from a specific institution. By leveraging data from multiple sources, the federated model can identify a wider variety of Marfan Syndrome manifestations, making it more reliable in diagnosing patients with different characteristics. This collaborative approach ultimately enhances the diagnostic process, allowing for more accurate assessments of Marfan Syndrome severity and abnormalities, while maintaining the privacy and integrity of patient data.
Advanced imaging techniques
Following are the advanced imaging techniques commonly used to assess the severity of cardiovascular manifestations in Marfan Syndrome patients:
Echocardiogram: This test uses ultrasound to create images of the heart, focusing on detecting aortic dilation or aneurysms-common cardiovascular manifestations in Marfan Syndrome.
MRI or CT scan: These imaging techniques are used to assess the aorta and other connective tissues, providing detailed views of abnormalities that cannot be detected through basic evaluations.
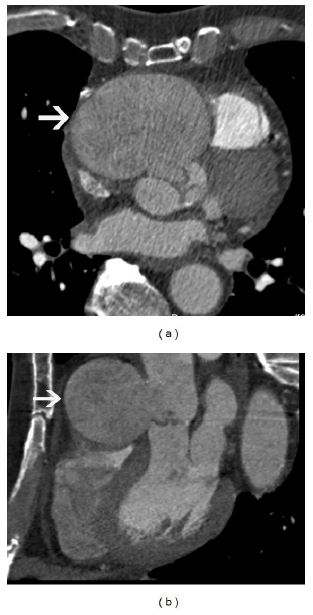
Figure 2 displays MRI scan images illustrating aortic root dilation, a critical cardiovascular manifestation of Marfan Syndrome. These advanced imaging tests help in accurately assessing the severity of the condition.
Datasets
Through our collaboration with The Marfan Foundation, we gained access to a comprehensive dataset of 12,826 patient records. These records include a diverse range of data, providing an extensive resource for developing models to detect and monitor Marfan Syndrome. To ensure privacy and security, we implemented federated learning across two nodes, each with its own subset of this data:
Node A: Echocardiogram and genetic data
Echocardiogram data: Node A contains approximately 4,200 records of detailed echocardiograms. These focus on identifying key cardiovascular manifestations, such as aortic root dilation and aneurysms, which are critical for predicting potential complications like aortic dissection.
Genetic data: Node A also holds 2,800 genetic records that highlight mutations in the FBN1 gene. These genetic insights are crucial for understanding the hereditary factors contributing to Marfan Syndrome and their correlation with clinical outcomes.
Node B: MRI/CT scans and clinical longitudinal data
MRI and CT scan data: Node B includes over 3,500 records of high-resolution MRI and CT scans. These scans provide in-depth views of the aorta and other connective tissues, facilitating early detection of abnormalities that are not visible through standard imaging techniques.
Clinical and longitudinal data: Additionally, Node B holds more than 2,300 records containing longitudinal follow-up information. This allows us to track disease progression over time and identify patterns or risk factors associated with worsening symptoms or complications.
By distributing this data across two nodes and applying federated learning, we ensure that patient privacy is maintained while still enabling the development of highly accurate and generalized models. The federated learning process allows both nodes to contribute to a global model without sharing raw data, leveraging the strengths of each node’s dataset. This collaborative approach has been instrumental in refining our models for more precise and early detection of Marfan Syndrome, which is essential for improving patient outcomes and preventive care.
Experiments and results
The experiments were divided into two phases corresponding to the two diagnostic stages: Basic Physical Evaluation and Specialized Diagnostic Tests.
Basic physical evaluation results
For the basic physical evaluation, we trained a CNN model to classify images as either “with Marfan Syndrome” or “without Marfan Syndrome.” The dataset used for training included images simulating common physical manifestations of Marfan Syndrome.
Table 1: Expanded confusion matrix table for basic physical evaluation.
| Experiment | True Positives (TP) | False Positives (FP) | False Negatives(FN) | True Negatives(TN) | Precision | Recall | Accuracy |
|---|---|---|---|---|---|---|---|
| Exp 1 | 92 | 10 | 8 | 150 | 0.90 | 0.92 | 0.92 |
| Exp 2 | 88 | 12 | 10 | 148 | 0.88 | 0.90 | 0.91 |
| Exp 3 | 95 | 8 | 7 | 155 | 0.92 | 0.93 | 0.94 |
| Exp 4 | 90 | 11 | 9 | 149 | 0.89 | 0.91 | 0.92 |
Metrics
Model Training: The CNN model was trained on a dataset that included images simulating the common physical manifestations of Marfan Syndrome, such as elongated limbs, scoliosis, and facial features.
Experiment results: Multiple experiments were conducted to assess the performance of the model, with each experiment evaluating key metrics, including True Positives (TP), False Positives (FP), False Negatives (FN), and True Negatives (TN).
Precision: The model demonstrated a strong ability to minimize false positives, with precision values ranging from 88% to 92%.
Recall: The model’s recall values indicated that it was effective in identifying true cases of Marfan Syndrome, with scores ranging from 90% to 93%.
Accuracy: The overall accuracy across experiments ranged from 91% to 94%, highlighting the model’s reliability in distinguishing between patients with and without Marfan Syndrome.
The classification task effectively filtered out patients who did not exhibit clear symptoms, minimizing the need for further testing. These results validate the CNN model’s potential for use in basic physical evaluations, allowing clinicians to identify patients with Marfan Syndrome based on physical manifestations with a high degree of confidence.
Specialized diagnostic tests
For the specialized diagnostic tests, we implemented a federated learning approach across two nodes to train YOLOv8 models. These models were used to detect key anatomical regions affected by Marfan Syndrome, such as the aortic root, aortic arch, lens dislocation, and spinal deformities. Federated learning enabled the two nodes to collaboratively train the model while keeping their local data private. The aggregated YOLOv8 model demonstrated superior performance over the previous-generation YOLOv5 models, with improvements in detection accuracy and computational efficiency.
The federated learning experiment involved two nodes, Node A and Node B, each containing local datasets. These datasets consisted of images simulating the physical manifestations of Marfan Syndrome, such as elongated limbs, scoliosis, and facial features.
In each training round, the local YOLOv8 models were trained independently on each node’s data. After training, the model weights were securely shared and aggregated using a federated averaging algorithm. This aggregated model was then distributed back to both nodes for the next round of training. This cycle of local training followed by global aggregation continued over several rounds, allowing the model to progressively improve its performance.
Table 2: Expanded Confusion Matrix Table for Specialized Diagnostic tests.
| Experiment | Node | True positives (TP) | False positives (FP) | False negatives (FN) | True negatives (TN) | Precision | Recall | Accuracy |
|---|---|---|---|---|---|---|---|---|
| Exp 1 | A | 92 | 10 | 8 | 150 | 0.90 | 0.92 | 0.92 |
| Exp 1 | B | 91 | 11 | 9 | 148 | 0.89 | 0.91 | 0.91 |
| Exp 1 | Federated | 94 | 8 | 6 | 153 | 0.92 | 0.94 | 0.94 |
| Exp 2 | A | 88 | 12 | 10 | 148 | 0.88 | 0.90 | 0.91 |
| Exp 2 | B | 90 | 13 | 9 | 150 | 0.87 | 0.91 | 0.92 |
| Exp 2 | Federated | 92 | 9 | 7 | 154 | 0.91 | 0.93 | 0.93 |
| Exp 3 | A | 95 | 8 | 7 | 155 | 0.92 | 0.93 | 0.94 |
| Exp 3 | B | 93 | 9 | 8 | 153 | 0.91 | 0.92 | 0.93 |
| Exp 3 | Federated | 97 | 7 | 6 | 157 | 0.93 | 0.94 | 0.95 |
| Exp 4 | A | 90 | 11 | 9 | 149 | 0.89 | 0.91 | 0.92 |
| Exp 4 | B | 88 | 12 | 10 | 147 | 0.88 | 0.90 | 0.91 |
| Exp 4 | Federated | 91 | 10 | 7 | 152 | 0.90 | 0.93 | 0.93 |
Metrics
Precision: The federated model demonstrated improved precision, with values reaching up to 93%, showing a reduction in false positives.
Recall: The recall scores improved in the federated model, with values up to 94%, indicating enhanced effectiveness in identifying true cases of Marfan Syndrome.
Accuracy: The accuracy of the federated model ranged from 93% to 95%, marking a clear improvement over the individual node models, which had accuracies ranging from 91% to 94%.
The federated learning approach not only ensured data privacy but also enhanced the YOLOv8 model’s performance by leveraging the strengths of data from multiple sources. These improvements in accuracy validate the potential of federated learning for training diagnostic models, making them more reliable and effective in clinical applications.
Discussion
Our literature review identified significant gaps in diagnosing and managing Marfan Syndrome, including the need for improved diagnostics, psychological support, and long-term monitoring. Studies [1-3] emphasized reduced physical fitness, the role of nitric oxide in aortic disease, and the impact of chronic pain. Research [4-6] highlighted the challenges of phenotypic variability in diagnosis, potential therapeutic targets, and the importance of continuous imaging. Studies [7-10] revealed issues such as underdiagnosis, discrepancies in monitoring, and the link between sleep apnea and cardiovascular mortality.
Furthermore, we highlighted the significant potential of Artificial Intelligence (AI) in enhancing Marfan Syndrome (MFS) detection and diagnosis. By implementing a two-stage diagnostic process-comprising a Basic Physical Evaluation using a Convolutional Neural Network (CNN) and Specialized Diagnostic Tests utilizing federated learning-the research addresses the challenges of early and accurate diagnosis.
The CNN model effectively identified key physical signs of Marfan Syndrome, such as elongated limbs and chest deformities, during the initial screening phase. This enabled early detection without the need for costly or invasive tests, making the model scalable and accessible. The model achieved precision between 88% and 92%, recall from 90% to 93%, and accuracy ranging from 91% to 94%, demonstrating strong potential for routine screenings.
For high-risk patients identified during the basic evaluation, the YOLOv8 models, trained through federated learning, were highly effective in detecting specific anatomical abnormalities. These models demonstrated precision up to 93%, recall up to 94%, and accuracy ranging from 93% to 95%. Federated learning allowed collaboration among multiple institutions while preserving patient data privacy, reducing bias from localized datasets, and making the model more generalized and reliable across diverse populations.
Conclusion
This study proposed a two-stage AI-driven model for detecting Marfan Syndrome, combining non-invasive physical evaluations with advanced diagnostic testing. The model demonstrated strong accuracy, precision, and recall in both screening and diagnostic phases. The CNN model performed well in identifying physical symptoms, while the YOLOv8 models enhanced detection accuracy for critical anatomical features, contributing to improved patient outcomes.
The integration of federated learning ensured data privacy while improving model performance across diverse populations, making the model more reliable and effective in clinical applications. With precision up to 93%, recall up to 94%, and accuracy reaching 95%, the proposed approach shows significant promise for early diagnosis and resource optimization.
Future work will focus on expanding the dataset, incorporating data from additional medical institutions, and further refining the model to enhance its generalizability and effectiveness. Additionally, integrating the model into clinical workflows and telemedicine platforms will enable broader access to early Marfan Syndrome detection, ultimately improving patient outcomes and reducing mortality associated with this complex genetic disorder.
References
- J Warnink-Kavelaars, L E d Koning, A E v d Hulst, A I Buizer, N Poissonnier, et al. Physical fitness in children with Marfan and Loeys-Dietz syndrome: Associations between cardiovascular parameters, systemic manifestations, fatigue, and pain, European Journal of Pediatrics. 2024; 183: 2421-2429.
- A d l Fuente-Alonso, M Toral, A Alfayate, M J Ruiz-Rodríguez, E Bonzón-Kulichenko, et al. Aortic disease in Marfan syndrome is caused by overactivation of sGC-PRKG signaling by NO, Nature Communications. 2021; 12: 1-13.
- Xf Lin, Lf Xie, Zf Zhang, J He, Yl Xie, et al. Quality of life in young patients with acute type A aortic dissection in China: Comparison with Marfan syndrome and non-Marfan syndrome, BMC Cardiovascular Disorders. 2024; 24: 1-8.
- M Karaoglan, G Nacarkahya, E H Aytac, M Keskin. Genotype and clinical phenotype of children with Marfan syndrome in Southeastern Anatolia, European Journal of Pediatrics. 2024; 183: 3219-3232.
- F Zhang, K Yao, Y Liu, M Zhou, Y Zhang, et al. Complement C3a/C3aR inhibition alleviates the formation of aortic aneurysm in Marfan syndrome mice, BMC Cardiovascular Disorders. 2024; 24: 1-12.
- A Lenz, M Warncke, F Wright, J M Weinrich, B P Schoennagel, et al. Longitudinal follow-up by MR angiography reveals progressive dilatation of the distal aorta after aortic root replacement in Marfan syndrome, European Radiology. 2023; 33: 6984-6992.
- N L Beetz, T D Trippel, K Philipp, C Maier, T Walter-Rittel, et al. Gehle, Discrepancy of echocardiography and computed tomography in initial assessment and 2-year follow-up for monitoring Marfan syndrome and related disorders, Scientific Reports. 2022; 12: 1-11.
- A Velandia-Sánchez, C A Polanía-Sandoval, J Senosiain-González, J V Álvarez-Martínez, S Gallo-Bernal, et al. Challenges in prompt identification and surgical correction of Marfan Syndrome aortic disease in a middle-income country: A case series study, Journal of Cardiothoracic Surgery. 2024; 19: 1-13.
- E O Klemenzdottir, G A Arnadottir, B O Jensson, A Jonasdottir, H Katrinardottir, et al. A population-based survey of FBN1 variants in Iceland reveals underdiagnosis of Marfan syndrome, European Journal of Human Genetics. 2024; 32: 44-51.
- N Gessler, P Wohlmuth, O Anwar, E S Debus, C Eickholt, et al. Sleep apnea predicts cardiovascular death in patients with Marfan syndrome: A cohort study, EPMA Journal. 2022; 13: 451-460.
- Ortho Marfan Syndrome. 2021. https://www.orthobullets.com/pediatrics/4089/marfan-syndrome.