SciBase Journals
SciBase Cardiology
ISSN 2996-4547
- Article Type: Case Report
- Volume 2, Issue 2
- Received: Sep 02, 2024
- Accepted: Oct 04, 2024
- Published Online: Oct 11, 2024
Effect of Alcohol on Heart: A Patient with Alcoholic Cardiomyopathy and Holiday Heart Syndrome
Christian Toquica1; Quang Dat Ha2*; Ramneek Sandhu2; Prami Nakarmi2; Bhavin Patel2; Kirit Patel, MD, FACC3
1Trinity Health Oakland Cardiovascular Fellow, USA.
2Internal Medicine Department, Trinity Health Oakland Hospital, USA.
3Cardiovascular Disease Fellowship/Wayne State University Program at Trinity Health Oakland, USA.
*Corresponding Author: Quang Dat Ha
Internal Medicine Department, Trinity Health Oakland
Hospital, USA.
Email: datquangha@gmail.com
Abstract
Alcohol use has been linked to the development of cardiac arrhythmias and non-ischemic dilated cardiomyopathy. We describe a case of a 29-year-old male who presented with palpitations and chest pain after binge drinking alcohol. We report the clinical presentation, investigations and outcomes after 6 months of abstinence from alcohol.
Citation: Toquica C, Dat Ha Q, Sandhu R, Nakarmi P, Patel B. Effect of Alcohol on Heart: A Patient with Alcoholic Cardiomyopathy and Holiday Heart Syndrome. SciBase Cardiol. 2024; 2(2): 1013.
Background
Alcohol is one of the most widely available recreational drugs in the United States of America. It is estimated that 17.6 million people have some type of alcohol use disorder and this has been linked to multiple health problems including cardiovascular disease [1]. When consumed in moderation, alcohol has several health benefits involving cardiovascular protection by reducing platelet aggregation through activation of the fibrinolytic system, increasing the High-Density Lipoproteins (HLD) and ApoA-I and ApoA-II levels, and the phenolic compounds in wine regulate and inhibit secretion of pro-inflammatory cytokines preventing endothelial dysfunction. These beneficial cardiovascular effects of alcohol are known as the “French paradox” [2]. Despite this, alcohol abuse can lead to several cardiovascular and metabolic diseases including cardiac arrhythmias and nonischemic dilated cardiomyopathy [3].
Objective
To describe a case with alcoholic cardiomyopathy and the physiological effects of alcohol on the heart.
To emphasize the early diagnosis and interventions in patients with alcoholic cardiomyopathy that have an impact on partial or complete recovery of cardiac function.
Case presentation
29-year-old male with no past medical history presented to the emergency department for one-day onset of palpitations and chest pain. The patient had prior episodes of palpitations that occurred after binge drinking. The patient endorsed drinking up to 40 cans of 8oz beer a day in intervals of 2 or 3 months for the past 8 years. There was no significant family history of cardiovascular disease. On admission, blood pressure: 167/98 mmHg, pulse: 143 beats/min, respiratory rate: 20/min, O2 Sat: 98% on room air, temperature: 98.5 Fahrenheit, and New York Heart Association (NYHA) class II-III. Cardiovascular examination was remarkable for tachycardia, and irregularly irregular pulse. There was no jugular venous dilation or pedal edema.
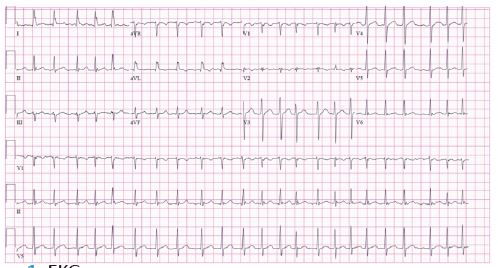
The EKG showed Atrial Fibrillation (AF) with rapid ventricular response and no ST changes (Figure 1).
Treatment was initiated with diltiazem and heparin infusions, achieving rate control after the few hours. Other investigations included: TSH 1.203 μIU/mL (0.465-4.680), T4 free 1.14 ng/mL (0.79-2.35), RPR non-reactive, troponins 0.03 ng/mL (Cutoff 0.12 ng/mL), normal urine and plasma metanephrine level and negative urine toxicology. An echocardiogram showed a Left Ventricular Ejection Fraction (LVEF) of 35%, moderate global hypokinesis, concentric LVH, enlarged left ventricular cavity, left atrium size 5.4 cm, dilated right atrium, dilated right ventricle, Right ventricular systolic pressure (RVSP) 24 mmHg, dilated aortic root 4.3 cm, mild-moderate mitral regurgitation, trace tricuspid regurgitation and normal aortic valve (Figure 2).

After day 3 of hospitalization, he underwent direct current cardioversion with 200 joules after a transesophageal echocardiogram. The patient returned to sinus rhythm and oral amiodarone was initiated. On day 5 the patient had a left heart catheterization which showed no narrow coronary arteries. Upon discharge, heparin infusion was changed to rivaroxaban. He was provided with a wearable cardioverter defibrillator given his severely decreased cardiac function and guideline-directed medical therapy was started with carvedilol 3.125 mg twice daily and lisinopril 10 mg once daily. The patient was seen for follow-up at 4 months having complete resolution of his symptoms. He remained abstinent from alcohol. A multiple gated acquisition scan showed no enlargement of the heart’s cavities and an improvement of his LVEF to 61%.
Discussion
Excessive alcohol consumption has been listed as the main cause of premature mortality in the US [4] and plays an enormous burden in the development of cardiac arrhythmias. Binge drinking is defined as a pattern of drinking that raises one’s blood ethanol concentration (BAC) to 0.08 g/dL or higher, it is commonly seen as a social phenomenon in which 25% of US adults participate every month [1].
The term ‘’Holiday heart syndrome’’ since its description in 1978 by Philip Ettinger was defined as the development of a supraventricular tachyarrhythmia, most frequently atrial fibrillation, in patients with no apparent or known cause of heart disease after an episode of heavy alcohol intake [5].
The physiological effects of alcohol are dose and time-dependent. Consumption of more than 5 drinks in men or 4 drinks in women in 2 hours or less has been shown to bring a person’s BAC to 0.08g or higher [6]. At these levels, alcohol causes acute myocardial effects including temporary depression of the LVEF [7], impairment in cardiac contractility, disturbances of cardiac rhythm, and elevations of blood pressure [3]. The mechanism through which alcohol causes arrhythmias appears to be related to intramyocardial release of catecholamines in response to acetaldehyde, electrolyte disturbances, and by decreasing the right atrium effective refractory period [3,8]. This has also been shown in a recent meta-analysis where they found that moderate and high levels of alcohol intake are associated with increased incident of AF, no significant increase was seen in low levels of alcohol consumption [9].
In contrast, chronic alcohol abuse causes a reduction in protein synthesis of structural and non-structural heart proteins that ends in apoptosis and necrosis. Ethanol gets converted into acetaldehyde and ethyl esters which produce excess free radicals. These free radicals cause oxidative stress in the myocytes and interfere with critical processes such as mitochondrial function and the activity of contractile proteins, translating into remodeling with hypertrophy and fibrosis [10]. These effects have been linked with AV dysfunction, arrhythmias, dilated cardiomyopathy, heart failure and sudden cardiac death [11].
Alcoholic cardiomyopathy (ACM) is the leading cause of secondary dilated cardiomyopathy; it encompasses 1/3 of all cases of non-ischemic dilated cardiomyopathy. ACM is defined as a dilated cardiomyopathy seen in patients with a consumption of >80 g of ethanol per day for at least 5 years [12]. Remarkably, an early diagnosis and alcohol abstinence may produce partial or complete recovery of cardiac function [13].
The presenting symptoms of ACM resemble those of congestive heart failure on any etiology, including shortness of breath on exertion, bilateral pitting edema, orthopnea, fatigue, oliguria and nocturia, and signs such as elevated jugular venous pressure, presence of S3 or S4, or a systolic murmur. A complete history including quantifying the amount of alcohol consumption and exclusion of other causes of dilated cardiomyopathy is key. Echocardiography is mandatory for diagnosing this condition and excluding other causes. The presence of biventricular chamber dilation and systolic-diastolic dysfunction is typically seen. Usually, a coronary angiography may be warranted to exclude contributing coronary artery disease [3].
The treatment of the ACM (Alcoholic cardiomyopathy) is not different from the standard treatment recommended for dilated cardiomyopathy. The ESC Guidelines recommend the use of diuretics to reduce cardiac preload and ACEi/ARBs or beta blockers to reduce post-load [14].
Abstinence from alcohol is the cornerstone to prevent further structural damage and decrease the risk of recurrence of AF. Further recommendations include reducing dietary sodium intake, and correcting of nutritional deficiencies including vitamin B6, folate, and B12 [15].
The use of ICD implant has been shown to decrease mortality in patients with nonischemic dilated cardiomyopathy who have decreased LVEF ≤35%, and an NYHA functional Class II or III. This mortality benefit is achieved through the prevention of sudden cardiac death [14].
Conclusion
We present a case of alcohol-induced cardiomyopathy and holiday heart syndrome from binge drinking. Patients who remain abstinent from alcohol may have a partial or complete recovery of cardiac function. Early diagnosis and interventions in these patient populations should follow the current up-to-date guideline therapies.
References
- National Council on Alcoholism and Drug Dependence, Inc. 2021. http://www.ncadd.org/about-addiction/alcohol/facts-about-alcohol.
- Fragopoulou E, Antonopoulou S. The French paradox three decades later: Role of inflammation and thrombosis. Clin Chim Acta. 2020; 510: 160-169. doi: 10.1016/j.cca.2020.07.013.
- Day E, Rudd JHF. Alcohol use disorders and the heart. Addiction. 2019; 114(9): 1670-1678. doi: 10.1111/add.14703.
- Stahre M, Roeber J, Kanny D, Brewer RD, Zhang X. Contribution of Excessive Alcohol Consumption to Deaths and Years of Potential Life Lost in the United States. Prev Chronic Dis. 2014; 11: 130293. DOI: http://dx.doi.org/10.5888/pcd11.130293.
- Ettinger PO, Wu CF, De La Cruz CJr, Weisse AB, Ahmed SS, et al. Arrhythmias and the Holiday Heart: Alcohol-associated cardiac rhythm disorders. Am Heart J. 1978; 95(5): 555-62.
- Fillmore MT, Jude R. Defining binge drinking as five drinks per occasion or drinking to a .08% BAC: Which is more sensitive to risk? Am. J. Addict. 2011; 20: 468-475.
- Guarnieri T, Lakatta EG. Mechanisms of myocardial contractile depression by clinical concentration of ethanol; study in ferret papillary muscles. J. Clin. Invest. 1990; 85: 1462-1467.
- Tonelo D, Providência R, Gonçalves L. Holiday heart syndrome revisited after 34 years. Arq Bras Cardiol. 2013; 101(2): 183-189. doi:10.5935/abc.20130153.
- Gallagher C, Hendriks JML, Elliott AD, Wong CX, Rangnekar G, et al. Alcohol and incident atrial fibrillation - A systematic review and meta- analysis. Int J Cardiol. 2017; 246: 46-52.
- Maisch B. Alcoholic cardiomyopathy: The result of dosage and individual predisposition. Herz. 2016; 41(6): 484-93. doi: 10.1007/s00059-016-4469-6.
- Fernández-Solà J. The Effects of Ethanol on the Heart: Alcoholic Cardiomyopathy. Nutrients. 2020; 12(2): 572. doi: 10.3390/nu12020572.
- George A, Figueredo VM. Alcoholic cardiomyopathy: a review. J Card Fail. 2011; 17(10): 844-9. doi: 10.1016/j.cardfail.2011.05.008.
- Mirijello A, Tarli C, Vassallo GA, Sestito L, Antonelli M, et al. Alcoholic cardiomyopathy: What is known and what is not known. Eur J Intern Med. 2017; 43: 1-5. doi: 10.1016/j.ejim.2017.06.014.
- McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, et al. ESC Scientific Document Group. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021; 42(36): 3599-3726. doi: 10.1093/eurheartj/ehab368.
- Voskoboinik A, Kalman JM, De Silva A, Nicholls T, Costello B, et al. Alcohol abstinence in drinkers with atrial fibrillation. N Engl J Med. 2020; 382: 20-8.