SciBase Journals
SciBase Cardiology
ISSN 2996-4547
- Article Type: Research Article
- Volume 2, Issue 2
- Received: Sep 06, 2024
- Accepted: Oct 11, 2024
- Published Online: Oct 18, 2024
Does Early Life Stress by Heart Failure Cause Short Stature, Learning Disabilities and Increase Later Cardiovascular Risk in Children with Congenital Heart Disease? Could we prevent it with Propranolol Treatment in Early Infancy?
Buchhorn R1-3*; Willaschek C1
Caritas Hospital Bad Mergentheim, Clinic for Pediatric and Adolescent Medicine, Uhlandstraße 7, Bad Mergentheim, Germany.
University of Würzburg, Josef-Schneider-Straße 2, Würzburg, Germany.
Practice for pediatric and adolescent medicine, Am Bahnhof 1, 74670 Forchtenberg, Germany.
*Corresponding Author: Buchhorn R
Caritas Hospital Bad Mergentheim, Clinic for
Pediatric and Adolescent Medicine, Uhlandstraße
7, Bad Mergentheim, Germany.
Email: buchrein@gmail.com
Abstract
Introduction: Infants have the highest risk to die from heart failure, one of the most stressful life events in infancy. Moreover, this early life stress may have an impact on growth, neurodevelopment and later cardiovascular risk according the Developmental origins of health and disease (abbreviated DOHaD) approach.
Methods: We analyse the current long-term follow up data of 19 children who are treated with propranolol in early infancy for severe heart failure due to congenital heart disease. We include anthropometric measurements from the medical records for German children, in which height, weight and head circumferences were documented from birth up to the 5th year of life and the data of weight and height at their last examination with a mean age of 9.5±3.5 years. We further analyze 24-hours heart rate variabilities from 42 routine Holter ECG that are part of regular outpatient controls.
Results: Propranolol prevented a further preoperative decline of height Z-scores that is confirmed in a separate analysis of eight infants with down syndrome. The preoperative Propranolol treatment is characterized by subnormal heart rates and physiological vagus activities indicated by the HRV parameter rMSSD. During long-time follow up, the heart rates are in low normal range and heart rate variabilities (e.g. rMSSD) are normal on average. We can exclude a detrimental effect of Propranolol therapy of heart failure in infants due to congenital heart defects on head circumference growth, if our group reached head circumference z-scores at long-time follow up slightly above the values given in the literature.
Discussion: These important long-time follow up data after effective pharmacotherapy of early life stress due to heart failure in early infancy with propranolol demonstrate a beneficial effect on growth and heart rate variability that may have an impact on neurodevelopment and later cardiovascular risk, the most important indicators for quality of life after successful cardiac surgery of congenital heart defects.
Citation: Buchhorn R, Willaschek C. Does Early Life Stress by Heart Failure Cause Short Stature, Learning Disabilities and Increase Later Cardiovascular Risk in Children with Congenital Heart Disease? Could we prevent it with Propranolol Treatment in Early Infancy?. SciBase Cardiol. 2024; 2(2): 1015.
Introduction
“Developmental origins of health and disease (abbreviated DOHaD) is an approach to medical research factors that can lead to the development of human diseases during early life development. These factors include the role of prenatal and perinatal exposure to environmental factors, such as undernutrition, stress, environmental chemicals, etc”; (Wikipedia). According to the number of children exposed, current research focused on intrauterine growth restriction, childhood stunting by malnutrition [1] and Prematurity. However, this approach seems to be very important for infants with congenital heart disease who suffer from heart failure – one of the most stress full life events in infancy - affecting up to 3120000 children worldwide in 2019 [2].
The pathophysiology of early life stress is intensively investigated [3] and the detrimental effect of norepinephrine on neurodevelopment is well understood [4]. However, there are only a few data of norepinephrine levels and Heart Rate Variabilities (HRV) that indicates early life stress in these affected children. These objective measurements are very important to identify the high-risk infants and to proof the therapeutic interventions. The impact of early life stress indicated by norepinephrine levels and heart rate variability on neurodevelopment is documented in infants after premature birth [5,6]. In congenital heart disease, we measured the highest norepinephrine levels and lowest vagus acitivities indicated by the HRV parameter RMSSD in infants with univentricular hearts and hemodynamic significant septal defects, who suffer from severe heart failure [7]. Most of all, compared to infants without a down syndrome (N=38), we measured the highest norepinephrine level (1811 ± 506 ng/l versus 856 ± 151 ng/l*, p=0.02) and lowest heart rate variability (RMSSD: 10.9 ± 6.2 ms versus 15.4 ± 7.7 ms*, p=0.0286) in infants with down syndrome and severe heart failure due to congenital heart disease.
We introduced the beta blocker Propranolol for the treatment of infants with severe heart failure due to congenital heart disease in 1996, based upon our publications that show a significantly elevated norepinephrine levels and reduced heart rate variability in these infants [7,8]. Table 1 shows the effect of the current pharmacotherapy of heart failure in infants with congenital heart disease on neurohormonal activation and heart rate variability. Based upon prospective studies, only propranolol significantly decreases plasma renin activity and aldosterone levels and increase the reduced heart rate variability indicated by the parameters SDNN and RMSSD. In contrast diuretics and the ACE inhibitor enalapril significantly increase the plasma renin activities by more than 400%. However, despite significant clinical benefits indicated by Ross’s heart failure score in two prospective randomized trials [9,10] and despite an ongoing high mortality in infants with heart failure due to congenital heart defects in Germany [11] and worldwide [2], this new innovative treatment was not supported by the local, national and international opinion leaders in pediatric cardiology.
Today, there are only data about nutritional supplementation in infants with early life adversities, who show some improvements in linear growth that are associated with small improvements in child development [12]. There are no data about pharmacological interventions on early life stress.
In the current publication we analyze growth and heart rate variabilities in our beta blocker treated infants in the longtime follow up. In our analysis we focused on the effect of propranolol on linear growth as a marker of early life stress that have an impact on neurodevelopment [13-17].
Based upon 24 h heart rate variability measurements, we expect the missing link between growth and neurodevelopment by an imprinting effect of early life stress on the autonomic nervous system, which we call autonomic imprinting as recently published [18]. We include the HRV data of our patients during longtime follow up in the current analysis.
Table 1: The impact of pharmacotherapy in infants with heart failure on Ross’ Heart Failure Score, neurohormonal activation and 24 h-Heart Rate Variability in prospective trials.
| Parameter | Pharmacotherapy | ||
|---|---|---|---|
| Diuretics [9] (Frusemid) | ACE Inhibitor [19] (Enalapril) | Beta-blocker [9] (Propranolol) | |
| Prospektive Trials | |||
| Ross Heart Failure Score | -20%* | ±0% | -60%** |
| Norepinephrine | +91% | -21% | |
| Plasma Renin Activity | +406%** | +450%* | -52%** |
| Aldosterone | +58% | -59%* | |
| 24 h-Heart RateVariability | |||
| Heart Rate | 0% | -15%** | |
| SDNN | +47%** | ||
| rMSSD | +79%** | ||
T-test between baseline versus treatment data in prospective randomized trials: *P-value < 0.05; ** P-value < 0.01; ***P-value < 0.001; ns = not significant.
Material and methods
Subjects
After publication of the compassionate use trial with propranolol in 6 infants with severe heart failure, 10 infants in Göttingen were treated in the prospective randomized trial CHF-PRO- INFANT [9]. However, after the clinic management changed in 2002, this therapy was no longer possible in Göttingen.
Due to the rejection of this new therapeutic approach by the opinion leaders in pediatric cardiology, the therapy was subsequently carried out at a small children’s hospital in Bad Mergentheim without any research funding. In summary 42 infants with severe heart failure are treated within the last 28 years, 15 of them had a Down syndrome (Table 2), 3 had other genetic abnormalities. Four children with univentricular hearts died, all these children had an unbalanced atrioventricular septal defect together with down syndrome, who has the worst prognosis of all univentricular hearts [20].
For the current analysis, we only had access to the children, who are treated in Bad Mergentheim as indicated in table 2. Patients with spontaneous closure of the ventricular septal defect (N=3) and two patients who died have to be excluded for further analysis. The patients had their first cardiac surgery at an age of 6.0±1.9 month.
The anthropometric measurements were taken from the medical records for German children, in which height, weight and head circumferences were documented from birth up to the 5th year of life (U1: birth, U2: 3.-10 day, U3: 4.-5. Week, U4: 3.-4. month, U5:6.-7. Month, U6: 10. 12. month, U7: 21-24. month, U8: 46.-48. month, U9:60. – 64 month). We further include the data of weight and height at their last examination with a mean age of 9.5±3.5 years. For the calculation of percentiles and Z-scores we use the internet-based App Pedz (https://pedz.de/de/rechner.html) which include specific percentiles for children with down syndrome. For our analysis, we only use these specific percentiles and Z-scores for children with down syndrome!
Table 2: The group of infants with severe heart failure, who are treated with propranolol.
| Patients (N=43) | AVSD (N=21) | KomplexCHD biventricular repair(N=7) | Univentricular repair (N=12) | Spontanous VSD Closure (N=3) | Down Syndrome (N=15) |
|---|---|---|---|---|---|
| Göttingen (N=16) | 8 | 1 | 7 | 0 | 5 |
| Bad Mergentheim (N=27) | 13 (10) | 6 (6) | 5 (3) | 3 | 10 (8) |
| Chromosome abnormalities (N=22) | 15 (71%) | 3 (43%) | 4 | 0 | 15 |
| Mortality (N=4)Mortality (N=4) | 0 | 0 | 4 (33%) | 0 | 4 (27%) |
AVSD: infants with ventricular or atrioventricular septal defects.
The number in brackets indicate the patients who were available for this analysis
Control group: For controls, data from normal healthy children (N=85) were retrieved from a previous project investigating normal heart rate variabilities in children. Therefore, the data from these patients, who attended our outpatient clinic for exclusion of cardiac arrhythmia, was analysed retrospectively. The retrospective analysis was approved by the ethical board of our states medical chamber (Landesärztekammer Baden Württemberg) and previously published [21].
We further include the data of three children with congenital heart disease and Down syndrome (T21) treated with standard therapy (Digoxin, diuretics, ACE inhibitor) by other cardiologists in comparison to our beta blocker treated infants with severe heart failure due to congenital heart disease and Down syndrome.
Processing and analysis of 24-hour-Holter recordings
For analysis of 24-hours heart rate variability, we use the routine Holter ECG as part of regular outpatient controls. For the current analysis 42 Holter ECGs are available: 10 < 2 years of age, 10 between 2 and 4 years, 13 between 4 and 8 years and 9 older than 8 years (11.9 ±2-0 years).
Measurement and interpretation of HRV parameters in the current sample were standardized according to the Task Force Guidelines. Cardiac autonomic functioning was measured by a 24-hour Holter 12 bit digital ECG (Reynolds Pathfinder II, Spacelabs, Germany; 1024 scans/sec). All Holter recordings were reviewed by an experienced cardiologist and were edited to validate the system’s QRS labeling in order to exclude artifacts. Measures of HRV were calculated employing only normal to normal intervals.
For time domain measures, mean RR interval, resulting heart rate and the following HRV parameters were calculated as average hourly values and as 24-hour average values: mean 24-hours heart rate, square root of the mean of the sum of squares of differences between adjacent NNintervals (RMSSD) and the standard deviation of NN intervals (SDNN). RMSSD predominantly reflects changes in vagal tone.
Statistical analysis
All results were reported as mean ± Standard Deviation (SD). Parametric statistics were used for all comparisons as most variables were normally distributed. Patients were compared to the age matched control group of health children using an independent samples t-test for equality of means.
Ethics
The German Federal Institute for Drugs and Medical Devices (BfArM) and the local ethics committee approved the protocol of the CHF-Pro-Infant study, which was conducted in accordance with the Declaration of Helsinki II and the Note for Guidance on Clinical Investigation of Medicinal Products in children (CPMP 1997). The parent’s written consent was obtained. Today, Carvedilol (for children > 1year) and propranolol (for infants) are proven in prospective randomized heart failure trials without any advices for severe adverse events in children with congenital heart disease. In the current cases, the technical implementation of heart surgery and cardiac catheterization as well as therapy planning took place in the cardio thoracic university centers. The conversion of the therapy was discussed extensively with the parents and an oral consent was obtained.
Results
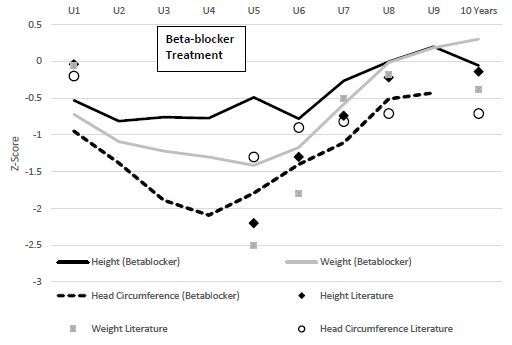
Growth parameters (Z-scores) of all 19 children with a preoperative beta blocker treatment of heart failure due to congenital heart disease are illustrated in Figure 1 at different ages from birth until 10 years of age, indicated by the medical records for German children (U1-U9) and the last visit at a mean age of 9.5±3.5 years, compared to the data as given in the literature [14,16]. Very low values of height, weight and head circumferences at birth indicate the high risk of our patient group due to the severity of the heart defect and the high portion of children with genetic abnormalities (Table 2). However, there is only a small further preoperative decline of weight and most of all height z-scores in the beta-blocker treated infants compared to the values as given in the literature. In contrast, the head circumference z-scores are very low in our patient group but all growth parameters (z-scores) of the beta blocker treated infants show a significant catch-up growth of all three parameters with comparable z-scores at an age of 5 (U9) to 10 years.
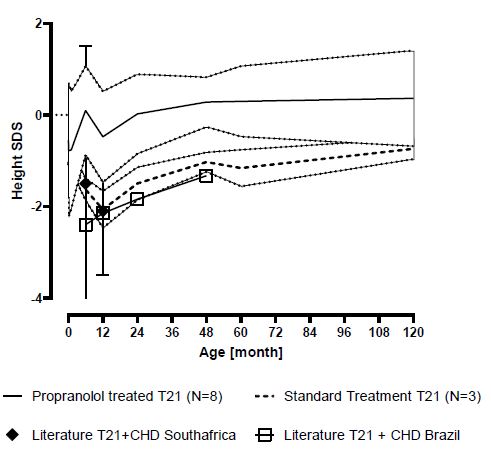
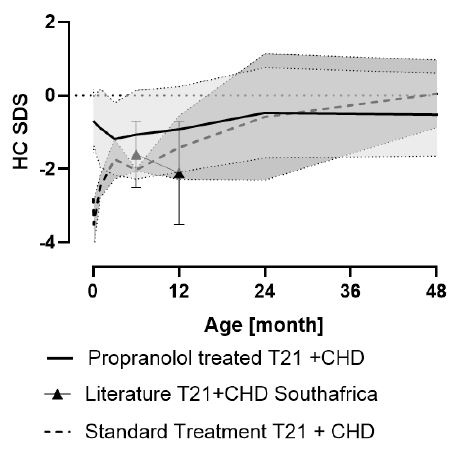
In order to form a uniform, more comparable group, we grouped the eight infants with down syndrome and atrioventricular septal defects together as shown in Figure 2. The growth parameter height z-scores of our infants with preoperative beta blocker treatment of heart failure due to congenital heart disease and Down syndrome (T21) at different ages from birth until 10 years of age, indicated by the medical records for German children (U1-U9) and the last visit at a mean age of 9.2±2.3 years, compared to the data of three children with congenital heart disease and Down syndrome (T21) treated with standard therapy (Digoxin, diuretics, ACE inhibitor) by other cardiologists and data of children with Down Syndrome and congenital heart disease as given in the literature [14,22]. We found significant better height Z-scores in our beta-blocker treated infants with down syndrome that persist up to the tenth year of life compared to the other infants with down syndrome who only received standard therapy with digoxin, diuretics ± ACE inhibitors. The only comparable data of head circumference z-scores are given 6 months after cardiac surgery for the south African T21 group [14] who had lower head circumference z-scores (-2.1±1.4) compared to our beta blocker treated infants at the same time (U6: -1.2 ± 1.0). This value is comparable to the longitudinal data after congenital heart surgery from Switzerland at one year of age (Head circumference z-score: -0.82 (min. -1.82; max. 0.04) in children without genetic abnormalities who had significant higher head circumferences at birth (-0.2, min -0.92; max. 0.77).
However, in contrast to the catch up growth after cardiac surgery of congenital heart defects as given in the literature [23] our beta blocker treated infants show a short post operative decline of the height z-scores with one year (U6) in all children (Figure 1) and children with down syndrome (Figure 2) that is probably explained by the post operative termination of beta blocker treatment. However, the height z scores of the beta blocker treated infants remain higher for the complete follow up to the tenth year of life.
Head circumference z-scores in 8 children with septal defects and down syndrome as shown in Figure 3 remain in the low normal range in children who received propranolol in contrast to 3 comparable children who received standard therapy and children with congenital heart defect and down syndrome as given in the literature [14] who had microcephaly with a z-score around -2 up to the first year of life. However, after successful cardiac surgery the head circumference z-scores show a catch-up growth in children who received standard therapy.
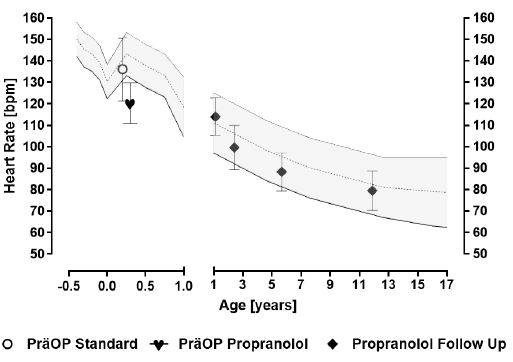
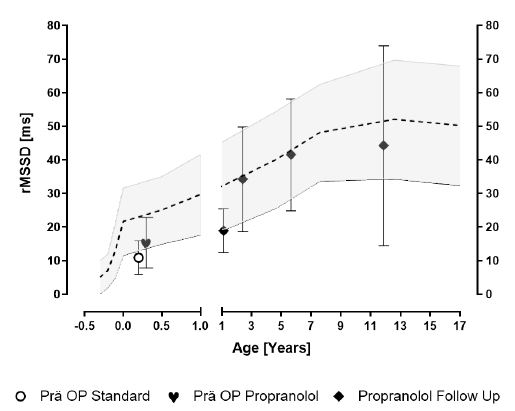
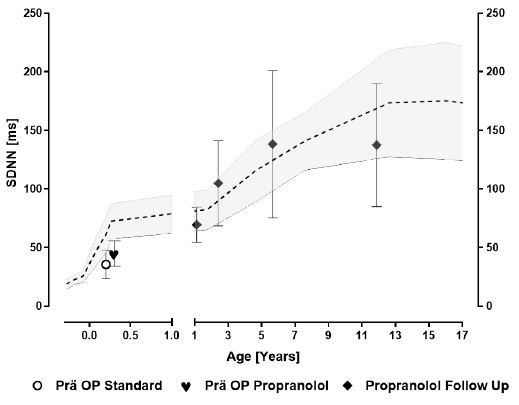
With respect to the Holter ECG data, we published the immediate preoperative effect of propranolol in infants with severe heart failure due to congenital heart defects on heart rate (Figure 4) and heart rate variability indicated by the vagus parameter RMSSD (Figure 5) [8]: Propranolol significantly decrease heart rate to subnormal values and increase Vagus activity (RMSSD) in the low normal range. The postoperative values at 1 year of age show heart rates in the high normal range and subnormal Vagus activities (RMSSD) after post operative completion of propranolol therapy. However, late postoperative Holter ECGs after 3 years of age show heart rates in the low normal range (Figure 4), normal global heart rate variabilities (SDNN; Figure 6) and Vagus activities (RMSSD, Figure 5) on average.
Discussion
The longtime analysis of growth parameters and heart rate variability of 19 children with severe heart failure due to congenital heart defects, who preoperatively received propranolol therapy demonstrate important beneficial effects:
Propranolol prevented a further preoperative decline of height Z-scores (Figure 1) that is confirmed in a separate analysis of the eight infants with down syndrome (Figure 2). After a short postoperative decrease of the height Z-scores due to termination of beta blocker treatment, the height z scores of the beta blocker treated infants remain higher for the complete follow up to the tenth year of life compared to children treated with standard therapy from literature.
The preoperative Propranolol treatment is characterized by subnormal heart rates and physiological vagus activities indicated by the HRV parameter rMSSD. After postoperative termination of beta blocker treatment, we observed an increase of heart rates in the high normal range (Figure 4) with low vagus activities (Figure 5, rMSSD). However, during longtime follow up the heart rates are in low normal range and Heart Rate Variabilities (e.g. rMSSD) are normal on average.
We can exclude a detrimental effect of Propranolol therapy of heart failure in infants due to congenital heart defects on head circumference growth, if our group reached head circumference z-scores at longtime follow up slightly above the values given in the literature (Figure 1). The head circumference z-scores of the eight infants with septal defects and Down syndrome who received propranolol is better compared to comparable infants who received standard therapy up to the first year of life (Figure 3).
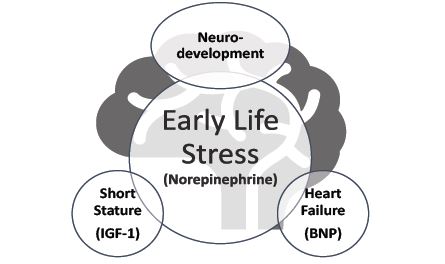
These observations may have an important impact on neurodevelopment and longtime cardiovascular risk according the Developmental origins of health and disease (abbreviated DOHaD) approach. This concept, how early stress from heart failure in infants with congenital heart defects have an immediate effect on height and a longtime effect on neurodevelopment is illustrated in Figure 7. We expect the missing link between growth and neurodevelopment by an imprinting effect of early life stress on the autonomic nervous system indicated by heart rate variability, which we call autonomic imprinting as recently published [18]. Our data based upon 24h heart rate variability measurements and all authors agree that nearly all children with operated congenital heart disease show reduced values during longtime follow up compared to their own healthy control group [24-30]. Recently, Toyofuku A. et al found a link between lower heart rate variability and cognitive impairments in children with congenital heart disease [31]. The complete recovery of heart rate variability during longtime follow up in our group of children who was treated with propranolol for severe heart failure in infancy open new opportunities to improve neurodevelopmental outcome in children with congenital heart disease.
We include the biomarkers IGF-1 for short stature, BNP for heart failure and norepinephrine for early life stress in Figure 7. The relationship between serum brain-type natriuretic peptide and IGF-1 is well documented in infants with shunt-dependent single ventricle [32]. Poor growth is well documented in children with congenital heart disease worldwide [16,33] and has a significant impact on neurodevelopmental outcome [13-17] that may be more pronounced in children with additional Down syndrome [22]. The most important risk factor for stunting in children with congenital heart diseases is congestive heart failure indicated by a Ross Score > 7 (OR 4.34 CI 2.00-4.64) [34]. Linear growth in heart disease with left to right shunts is related to insulin-like growth factor-1 and improve after surgical intervention [23]. The relationship between growth and intelligence quotient is well documented in children with Down syndrome [35] and seems to be related to IGF1 deficiency [36].
Our observation may have a further impact on longtime cardiovascular risk in patients with congenital heart disease, if it is confirmed that the drop of heart rate variability in patients with congenital heart disease can be prevented by an effective therapy of early life stress with propranolol in infancy. The enhanced cardiovascular risk of patients with operated congenital heart disease is well documented [37], even in adults with lower-complexity congenital heart disease without residual defects that is not well understood [38]. Resting heart rate is a proven indicator of the enhanced cardiovascular risk in adults with operated congenital heart disease [39]. Our data indicates 24-hours heart rates in the low normal range after propranolol treatment in infancy (Figure 3).
Unfortunately, our longtime follow up data are limited of cause the missing data from the University hospital Göttingen and the lack of developmental neurological examination, which was not possible in our small children’s hospital and due to the lack of research funding. However, we are happy about the very good cognitive development of our children with down syndrome who are treated with propranolol for severe heart failure in early infancy in comparison to historical controls and children who only received standard therapy.
References
- Suryawan A, Jalaludin MY, Poh BK, et al. Malnutrition in early life and its neurodevelopmental and cognitive consequences: a scoping review. Nutr Res Rev. 2022; 35(1): 136-49. doi: 10.1017/s0954422421000159
- Su Z, Zou Z, Hay SI, et al. Global, regional, and national time trends in mortality for congenital heart disease, 1990-2019: An age-period-cohort analysis for the Global Burden of Disease 2019 study. E Clinical Medicine. 2022; 43: 101249. doi: 10.1016/j.eclinm.2021.101249
- Smith KE, Pollak SD. Early life stress and development: potential mechanisms for adverse outcomes. J Neurodev Disord. 2020; 12(1): 34. doi: 10.1186/s11689-020-09337-y
- Saboory E, Ghasemi M, Mehranfard N. Norepinephrine, neurodevelopment and behavior. Neurochem Int. 2020; 135: 104706. doi: 10.1016/j.neuint.2020.104706
- Dimitrijević L, Bjelaković B, Čolović H, et al. Assessment of general movements and heart rate variability in prediction of neurodevelopmental outcome in preterm infants. Early Hum Dev. 2016; 99: 7-12. doi: 10.1016/j.earlhumdev.2016.05.014
- Evans DJ, MacGregor RJ, Dean HG, et al. Neonatal catecholamine levels and neurodevelopmental outcome: A cohort study. Arch Dis Child Fetal Neonatal Ed. 2001; 84(1): F49-52. doi: 10.1136/fn.84.1.f49
- Buchhorn R, Kießling C, Wessel A, et al. Neurohumorale Aktivierung bei Patienten mit congenitalen Vitien- Einfluss des Lebensalters, des Herzfehlers und der Hämodynamik. Herz/Kreisl. 2000; 32: 22-28.
- Buchhorn R, Hulpke-Wette M, Nothroff J, et al. Heart rate variability in infants with heart failure due to congenital heart disease: reversal of depressed heart rate variability by propranolol. Med Sci Monit. 2002; 8(10): CR661-CR66.
- Buchhorn R, Hulpke-Wette M, Hilgers R, et al. Propranolol treatment of congestive heart failure in infants with congenital heart disease: The CHF-PRO-INFANT Trial. Congestive heart failure in infants treated with propanol. Int J Cardiol. 2001; 79(2-3): 167-73.
- Ramakrishnan S, Ghati N, Ahuja RS, et al. Efficacy and safety of propranolol in infants with heart failure due to moderate-to-large ventricular septal defect (VSD-PHF study) - A prospective randomized trial. Annals of pediatric cardiology. 2021; 14(3): 331-40. doi: 10.4103/apc.APC_94_21
- Abdul-Khaliq H, Gomes D, Meyer S, et al. Trends of mortality rate in patients with congenital heart defects in Germany-analysis of nationwide data of the Federal Statistical Office of Germany. Clinical research in cardiology: Official journal of the German Cardiac Society. 2024. doi: 10.1007/s00392-023-02370-6
- Prado EL, Larson LM, Cox K, et al. Do effects of early life interventions on linear growth correspond to effects on neurobehavioural development? A systematic review and meta-analysis. Lancet Glob Health. 2019; 7(10): e1398-e413. doi: 10.1016/s2214-109x(19)30361-4
- Smith R, Ntsiea V, Brown S, et al. Pre-operative neurodevelopmental assessment in young children undergoing cardiac surgery in central South Africa: feasibility and clinical value. Cardiovasc J Afr. 2022; 33(3): 145-52. doi: 10.5830/cvja-2021-057
- Robyn S, Veronica N, Stephen B, et al. Undernutrition in young children with congenital heart disease undergoing cardiac surgery in a low-income environment. BMC Pediatr. 2024; 24(1): 73. doi: 10.1186/s12887-023-04508-x
- Trivedi A, Browning Carmo K, Jatana V, et al. Growth and risk of adverse neuro-developmental outcome in infants with congenital heart disease: A systematic review. Acta Paediatr. 2023; 112(1): 53-62. doi: 10.1111/apa.16564
- Hapuoja L, Kretschmar O, Rousson V, et al. Somatic growth in children with congenital heart disease at 10 years of age: Risk factors and longitudinal growth. Early Hum Dev. 2021; 156: 105349. doi: 10.1016/j.earlhumdev.2021.105349
- Ravishankar C, Zak V, Williams IA, et al. Association of impaired linear growth and worse neurodevelopmental outcome in infants with single ventricle physiology: a report from the pediatric heart network infant single ventricle trial. J Pediatr. 2013; 162(2): 250-6.e2. doi: 10.1016/j.jpeds.2012.07.048
- Buchhorn R, Meint S, Willaschek C. The Impact of Early Life Stress on Growth and Cardiovascular Risk: A Possible Example for Autonomic Imprinting? PloS one. 2016; 11(11): e0166447. doi: 10.1371/journal.pone.0166447
- Steichert M, Cawello W, Bajcetic M, et al. Influence of Age, Heart Failure and ACE Inhibitor Treatment on Plasma Renin Activity in Children: Insights from a Systematic Review and the European LENA Project. FBL. 2023; 28(12) doi: 10.31083/j.fbl2812335
- Hadjicosta E, Franklin R, Seale A, et al. Cohort study of intervened functionally univentricular heart in England and Wales (2000-2018). Heart. 2022; 108(13): 1046-54. doi: 10.1136/heartjnl-2021-319677
- De Bock F, Jarczok MN, Hoffmann K, et al. Do our children lose vagus activity? Potential time trends of children’s autonomic nervous system activity. Int J Cardiol. 2013; 170(2): e30-e32.
- Bravo-Valenzuela NJ, Passarelli ML, Coates MV, et al. Weight and height recovery in children with Down syndrome and congenital heart disease. Rev Bras Cir Cardiovasc. 2011; 26(1): 61-8. doi: 10.1590/s0102-76382011000100013
- Soliman AT, Elawwa A, Khella A, et al. Linear growth in relation to the circulating concentration of insulin-like growth factor-I in young children with acyanotic congenital heart disease with left to right shunts before versus after surgical intervention. Indian J Endocrinol Metab. 2012; 16(5): 791-5. doi: 10.4103/2230-8210.100678
- Butera G, Bonnet D, Iserin L, et al. Total cavopulmonary and atriopulmonary connections are associated with reduced heart rate variability. Heart. 1999; 82(6): 704-7. doi: 10.1136/hrt.82.6.704
- Okólska M, Łach J, Matusik PT, et al. Heart Rate Variability and Its Associations with Organ Complications in Adults after Fontan Operation. Journal of clinical medicine. 2021; 10(19) doi: 10.3390/jcm101944
- Maagaard M, Eckerström F, Hjortdal VE. Cardiac Arrhythmias and Impaired Heart Rate Variability in Older Patients with Ventricular Septal Defects. Journal of the American Heart Association. 2021; 10(17): e020672. doi: 10.1161/jaha.120.020672
- Davos CH, Francis DP, Leenarts MF, et al. Global impairment of cardiac autonomic nervous activity late after the Fontan operation. Circulation. 2003; 108 Suppl 1: Ii180-5. doi: 10.1161/01.cir.0000087946.47069.cb
- Cansel M, Yagmur J, Ermis N, et al. Effects of transcatheter closure of atrial septal defects on heart rate variability. J Int Med Res. 2011; 39(2): 654-61. doi: 10.1177/147323001103900235
- Folino AF, Russo G, Bauce B, et al. Autonomic profile and arrhythmic risk stratification after surgical repair of tetralogy of Fallot. Am Heart J. 2004; 148(6): 985-9. doi: 10.1016/j.ahj.2004.07.003
- Alstrup M, Karunanithi Z, Maagaard M, et al. Sympathovagal imbalance decades after atrial septal defect repair: a long-term follow-up study. Eur J Cardiothorac Surg. 2021; 61(1): 83-89. doi: 10.1093/ejcts/ezab235
- Toyofuku A, Ehrler M, Naef N, et al. Heart rate variability and cognitive functions in adolescents with complex congenital heart disease. Pediatr Res. 2024. doi: 10.1038/s41390-024-03432-9
- Gardner MM, Faerber J, Glatz AC, et al. Relationship between Serum Brain-Type Natriuretic Peptide and Biomarkers of Growth in Infants with Shunt-Dependent Single Cardiac Ventricle. The American journal of cardiology. 2022; 171: 146-50. doi: 10.1016/j.amjcard.2022.01.052
- Daymont C, Neal A, Prosnitz A, et al. Growth in children with congenital heart disease. Pediatrics. 2013; 131(1): e236-42. doi: 10.1542/peds.2012-1157
- Okoromah CA, Ekure EN, Lesi FE, et al. Prevalence, profile and predictors of malnutrition in children with congenital heart defects: A case-control observational study. Arch Dis Child. 2011; 96(4): 354-60. doi: 10.1136/adc.2009.176644
- Kłosowska A, Kuchta A, Ćwiklińska A, et al. Relationship between growth and intelligence quotient in children with Down syndrome. Translational paediatrics. 2022; 11(4): 505-13. doi: 10.21037/tp-21-424
- Araya P, Kinning KT, Coughlan C, et al. IGF1 deficiency integrates stunted growth and neurodegeneration in Down syndrome. Cell Rep. 2022; 41(13): 111883. doi: 10.1016/j.celrep.2022.111883
- Dellborg M, Giang KW, Eriksson P, et al. Adults with Congenital Heart Disease: Trends in Event-Free Survival past Middle Age. Circulation. 2023; 147(12): 930-38. doi: 10.1161/circulationaha.122.060834
- Saha P, Potiny P, Rigdon J, et al. Substantial Cardiovascular Morbidity in Adults With Lower-Complexity Congenital Heart Disease. Circulation. 2019; 139(16): 1889-99. doi: 10.1161/circulationaha.118.037064
- Hendriks PM, Van den Bosch AE, Kors JA, et al. Heart rate: an accessible risk indicator in adult congenital heart disease. Heart. 2024; 110(6): 402-07. doi: 10.1136/heartjnl-2023-323233