SciBase Journals
SciBase Cardiology
ISSN 2996-4547
- Article Type: Research Article
- Volume 2, Issue 3
- Received: Oct 17, 2024
- Accepted: Nov 15, 2024
- Published Online: Nov 22, 2024
Utility of a Wireless Ambulatory Monitoring System for Arrhythmic Event Detection in Pediatric Patients
Fernando Centeno-Malfaz*; Carlos Alcalde-Martín; Beatriz Salamanza-Zarzuela
Pediatric Cardiology, Recoletas Salud Hospital, Campo Grande, Valladolid, Spain.
*Corresponding Author: Fernando Centeno-Malfaz
Pediatric Cardiology, Recoletas Salud Hospital, Campo
Grande, Valladolid, Spain.
Tel: +34-983135555;
Email: fernando.centeno@gruporecoletas.com
Abstract
Introduction: Detection of arrhythmias in asymptomatic patients or with intermittent clinics represent a diagnostic challenge, being the traditional 24-hour monitoring systems, with low diagnostic performance. The Nuubo® system is one of the new wireless ambulatory monitoring systems (SMAI), which allows recording cardiac activity for up to 30 days.
Methods: Prospective observational cohort study, in patients with structural cardiological diseases, arrhythmogenic disorders, clinical susceptible to arrhythmias and/or with potentially arrhythmogenic diseases. Comparing arrhythmogenic findings obtained between SMAI and conventional holter.
Results: We conducted 35 studies. The SMAI study time was 361.97 hours (SD 227.55), and 20.8 hours (SD1.77) with Holterconvecional. Ectopic beats only showed clinical correlation in one of the patients with palpitations. In one case, both supra and ventricular ectopics accounted for more than 3% of the beats, in a patient who also presented streaks of supraventricular tachycardia visible with both systems. Supraventricular tachycardia was found in a four-year-old patient who reported sudden chest pain. A patient with compacted cardiomyopathy and another in a study by presyncopes, presented streaks of unsuptamed monomorphic ventricular tachycardia, not detected in conventional holter.
Conclusion: The SMAI has allowed to confirm the presence of potentially lethal arrhythmias that had not been recorded in conventional systems. In symptomatic patients it allows monitoring until the presence of the referred clinic, and its subsequent evaluation, allowing the treatment of the arrhythmia or discarding the cardiac origin of the same.
Keywords: Holter-ECG; Arrhythmogenic events; Arrhythmias; Inhalambric ambulatory detection systems.
Citation: Centeno-Malfaz F, Alcalde-Martín C, Salamanza-Zarzuela B. Utility of a Wireless Ambulatory Monitoring System for Arrhythmic Event Detection in Pediatric Patients. SciBase Cardiol. 2024; 2(3): 1017.
Introduction
The detection of arrhythmias in asymptomatic patients or with intermittent clinics represent a diagnostic challenge in the Pediatric Cardiology consultation. In addition to the history, physical examination and electrocardiogram, holter ambulatory electrocardiograma (Holter ECG) monitoring during 24 hours is the most used method for analyzing heart rythm and arrhythmia, despite its poor diagnostic performance (12-30%), especially in patients with sporadic symptoms [1-4]. The Implantable Loop Repcrders (ILR) as invasive method, are and alternative for adults and pediatric patients, in whom the cause of syncoe or palpitations could not be establisehed despiete a full non invasive investigation [4-6]. One of the new wireless ambulatory monitoring systems (SMAI) is the Nuubo system® which consists of a textile breastplate with integrated electrodes, which adapts to the size and mobility of patients and has added a recorder that allows recording up to 30 days of cardiac recording. Today there are no published works on its use in pediatric patients. Our objetive comparing arrhythmogenic findings obtained between SMAI and conventional holter in pediatric patients with structural cardiological diseases, arrhythmogenic disorders, clinical susceptible to arrhythmias and/or with potentially arrhythmogenic diseases.
Material and methods
This is a single-center prospective study of patients under 16 years old at the Department of Pediatric Cardiology in a third level Hospital. Patients were included from 1 January 2019 to 31 December 2020. Patients with structural cardiological diseases (structural congenital heart disease or cardiomyopathies), arrhythmogenic disorders, posible clinic of cardiac origin and/or with systemic diseases with potential arrhythmic involvement are included. Patients will undergo both the conventional 24-hour holter-ecg and a Nuubo® SMAI registry. The objective was to compare the diagnostic performance between both techniques.
The preparation of the work has followed the rules established for this purpose by the Research Ethics Committee (CEIC) of the West Area of Valladolid. All patients and their legal guardians have received information about the study and have signed an informed consent prior to their participation.
Clinical trial registration are not applicable for your study.
Results
We examined 35 studies in 31 patients (mean age 10.14±3,85 years, between one month old and 16 years old). Mean study time was 361.97±227.55 hours with the SMAI system and 20.8±1.77 hours with holter-convecional.
The reasons for study were:
Six patients with structural heart disease and cardiomyopathies, at risk of developing arrhythmias (two men with Tetralogy of Fallot, one patient man with pulmonary atresia, two patients with coronary anomalies (one man, one female) and one patient man with uncompacted cardiomyopathy). Mean age 10.6±4.32 years.
12 patients diagnosed with primary arrhythmogenic diseases: six patients with congenital long Qt syndrome, one patient with short QT syndrome, one patient with Brugada syndrome, one patient with ectopic tachycardia of the junction, one patient with Wolf-Parkinson-White syndrome and two patients with paroxysmal supraventricular tachycardia history. Eight patients were female and six were male. Mean age 8.39±4.32 years.
12 symptomatic patients with clinical with possible cardiological origin where the cardiac etiology has not been ruled out or cataloged within other known pathologies. Seven women who presented palpitations clinic and two with repeated presyncopes; and three men, two of them with a palpitations clinic and one with a syncope with exercise. Mean age 11.75±2.28 years.
A one-month-old female patient diagnosed with tuberous sclerosis with multiple cardiac tuberomas, asymptomatic.
The age difference between the different groups was statistically significant. The registration time was significantly longer (P< 0,05) in asymptomatic patients (504±208.5 hours) than in symptomatic patients, in whom the system was removed at the time of appearance of the clinic (267±108.5 hours).
The following table (Table 1) shows the heart rates recorded with both methods. The maximum heart rate was significantly higher in the Nuubo system records.
The electrocardiographic alterations found are summarized in (Table 2). The most frequent finding was non-pathological sinus tachycardia in 100% of patients, followed by monomorphic Premature Supraentricular Contractions (PSVCs), monomorphic Premature Ventricular Contractions (PVCs), sinus pauses, Ventricular Tachycardia (VT) and Supra Ventricular Tachycardia (SVT).
The ectopic beats only showed clinical correlation in one of the patients under study due to palpitations. The rest of the PSVCs findings had no clinical correspondence, and due to their frequency and time of appearance were considered non-pathological.
Only in one case, with ectopic tachycardia of the junction, both SPVCs and SPVCs accounted for more than 3% of the beats, this patient also presented streaks of SVT visible in the two recording systems. The other finding of SVT corresponds to a four-year-old patient (Figure 1), with a normal 24 h record, who reported sudden onset and end chest pain, and who was diagnosed with preexcitation syndrome that required ablative treatment.
Two episodes of nonsustained monomorphic ventricular tachycardia were found in two male patients. A 13-year-old patient suffered from uncompacted cardiomyopathy (Figure 2) and was asymptomatic. The other patient, 8 years old, presented presyncopes. In neither case had this arrhythmia been detected with the conventional Holter-EKG system.
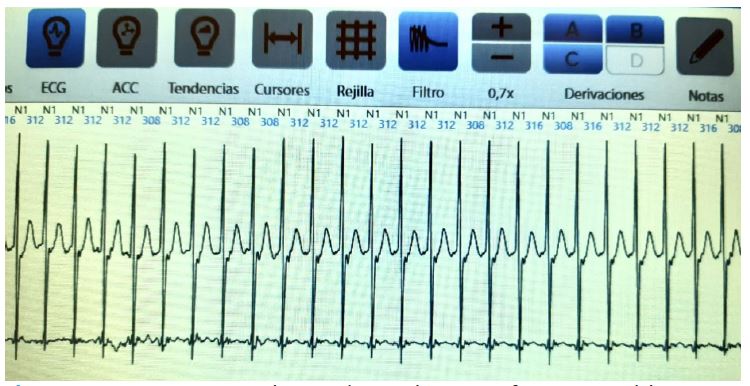
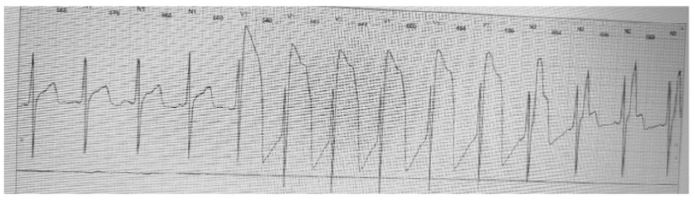
Table 1: Heart rates recorded with both methods.
| Convencional Holter-EKG | SMAI register | p | |
|---|---|---|---|
| Minimun heart rate (bpm) | 52 | 48 | >0,05 |
| Maximum heart rate (bpm) | 158 | 183 | < 0,05 |
| Mean heart rate (bpm) | 88 | 86 | >0,05 |
Table 2: Electrocardiographic alterations found with both methods.
| Convencional Holter-ECG (number of patients) | SMAI register (number of patients) | |
|---|---|---|
| Sinus pauses | 2 | 4 |
| PSVCs | 6 | 8 |
| PVCs | 6 | 6 |
| SVT | 1 | 2 |
| VT | 0 | 2 |
Discussion
The detection of arrhythmias in pediatric patients is a diagnostic challenge, despite which there are very few publications on the subject. Until now, holter ambulatory Electrocardiogram (ECG) monitoring, was, together with the ECG, the most used tool in pediatric patients for the detection of arrhythmic events. However, in addition to being unprofitable, due to the limitation of the time studied, it is sometimes uncomfortable for pediatric patients, since the devices are not designed either for that body size or for the activity of young patients. Implantable registration systems, on the other hand, are very effective in the diagnosis, especially of intermittent arrhythmias, but they are an invasive method, which we try to avoid in pediatric age. In recent years, new monitoring tools have emerged, such as the SMAI Nuubo®, which in addition to adapting to the size of the patient, allows to record the heart rate up to 30 days. With this new system, we have found higher maximum heart rates, which could be explained by performing physical activity during monitoring, which could not always be done with the conventional monitoring system due to the patient’s adaptation to the system. In this work, we have found advantages in two types of patients. On the one hand in patients with structural heart disease or cardiomyopathies who, due to their pathology, could present asymptomatic arrhythmias, and yet potentially lethal, in which the heart rhythm has been recorded for as long as possible. This group includes the patient with ectopic tachycardia of the junction, who presented multiple episodes of ventricular tauicardia. And the patient with uncompacted myocardiopathy in whom an episode of VT was detected. On the other hand, in patients with symptoms of possible cardiac origin, it allows to maintain the record until the appearance of these symptoms, being able to confirm or rule out the arrhythmogenic origin of the same. This is especially important in younger patients, who describe the symptoms non-specifically. As an example of these patients, the case of the eight-year-old patient with presincopes, which corresponded in the ECG trace with SVT. In this same group, of symptomatic patients, it should be noted that the rest of the patients could be discharged, when it was verified that the clinic they referred, did not correspond to any type of arrhythmia, presenting the rest of the normal cardiological study. Most of these patients had multiple normal 24-hour records, during which they had no symptoms.
There are few studies comparing conventional ECG monitoring with other monitoring tools. Patch ambulatory ECG monitors provided similar clinical impact as traditional monitors, but they more often provided results that allowed discharge from cardiology care [7]. This system allows you to register up to 7 days, compared to 30 in the Nuubo system. PocketECG system for continuous and real-time ECG recording is a reliable method for the assessment of heart rhythm and dysrhythmias in children and adolescents. In the same way as the system analyzed in this work, it allows to record the heart rate for several weeks. It also has the advantage that the pace is analyzed in real time [4]. The ZIO® XT Patch, is other tool, has cardiac monitoring capabilities that can be utilized for up to 14 days. It has shown good efficacy in the detection of cardiac events in pediatric age, although the work carried out with this system has been carried out in patients with an average age higher (mean age 12.7 years old) than that of this study (mean age 10.14 years old) [8]. Other Works shows equal quaility of the apple watch derived iECG compared to a lead 1 in 12-lead ECG in children. While de automatic IECG intrepretation by the internal algorithm seems to be insuficient in children, the iECG might be a primising option for the use al a mobile event monitoring for documentation of arrthymyas in childrensince four years-old [9]. Faced with these tools we find as the main advantage of the Nuubo system the ability to record up to 30 days, the quality of the record even during physical exercise and the possibility of carrying out the study in patients from the neonatal era. Unlike most of these systems, the system does not measure the Qt interval automatically.
Conclusion
The conclusion of this paper is the Nuubo wireless monitoring system is one of the new diagnostic tools that allow the detection of arrhythmic events in pediatric age. Its main advantages, compared to other diagnostic tools, are the possibility of use in patients from the neonatal period and the possibility of registration of up to 30 days.
Limitations
The stufy is limited because its single-center designs and the sample limited to the number of textil breastplate garments available for the study.
Authors’ contributions
The three authors who signed the article accept the publication of the article, having read, accepted and actively participated in the preparation of the article.
None of the authors have received funding for the realization of the work and are free of conflict of interest. The material for carrying out the work has been financed with a GRS grant from the castilla y León health system. All data is available
The preparation of the work has followed the rules established for this purpose by the Research Ethics Committee of the West Area of Valladolid. All patients and their legal guardians have received information about the study and have signed an informed consent prior to their participation.
Clinical trial registration are not applicable for this study.
References
- J Francisco-Pascual, et al. Rendimiento diagnóstico y evaluación económica de un protocolo diagnóstico basado en el uso sistemático de un registrador externo de eventos en asa cerrada en pacientes con palpitaciones. Rev Esp Cardiol. 2019; 72(6): 473-478.
- Hoefman E, Bindels P, Van Weert, H. Efficacy of diagnostic tools for detecting cardiac arrhythmias: Systematic literature search. Neth Heart J. 2010; 18: 543-551.
- Jonathan S. Steinberg MD. 2017 ISHNE-HRS expert consensus statement on ambulatory ECG and external cardiac monitoring/telemetry. Ann Noninvasive Electrocardiol. 2017; 22: e12447.
- Bieganowska K, Kaszuba A, Bieganowski M, et al. Pocket ECG: A New Noninvasive Method for Continuous and Real-Time ECG Monitoring-Initial Results in Children and Adolescents. Pediatr Cardiol. 2017; 38: 448-455.
- Rossano J, Bloemers B, Sreeram N, Balaji S, Shah MJ. Efficacy of implantable loop recorders in establishing symptom-rhythm correlation in young patients with syncope and palpitations. Pediatrics. 2003; 112(3 Pt 1): e228-33.
- Gass M, Apitz C, Salehi-Gilani S, Ziemer G, Hofbeck M. Use of the implantable loop recorder in children and adolescents. Cardiol Young. 2006; 16(6): 572-8.
- J Ryan Hitt, Elizabeth Carter, Joseph May. Patch versus traditional ambulatory ECG monitoring in children, Progress in Pediatric Cardiology. 2021; 101408.
- Pradhan S, Robinson JA, Shivapour JK, Snyder CS. Ambulatory Arrhythmia Detection with ZIO® XT Patch in Pediatric Patients: A Comparison of Devices. Pediatr Cardiol. 2019; 40(5): 921-924.
- Kobel M, Kalden P, Michaelis A, et al. Accuracy of the Apple watch iECG in Children With and without Congenital Heart Disease. Pediatr Cardiol. 2021.