SciBase Journals
SciBase Cardiology
ISSN 2691-7785
- Article Type: Case Report
- Volume 3, Issue 1
- Received: Jul 30, 2025
- Accepted: Aug 18, 2025
- Published Online: Aug 25, 2025
Percutaneous treatment of pulmonary artery pseudoaneurysm embolization after failed endovascular access: A case report and literature review
Van Cong Cung1,3; Van Luong Hoang1; Nhat Tam Tran1; Manh Cuong Vu1; Tuan Vu Le3; Quang Loc Tran2,3*
1Department of Diagnostic Imaging, National Lung Hospital, Vietnam.
2Department of Diagnostic Imaging, Viet Duc University Hospital, Vietnam.
3Department of Diagnostic Imaging, VNU University of Medicine and Pharmacy, Vietnam.
*Corresponding Author: Quang Lộc Trần
Department of Radiology, University of Medicine and
Pharmacy (VNU-UMP), Vietnam National University, Hanoi, Vietnam., Aveiro, Portugal.
Email: tranquangloc8396@gmail.com
Abstract
Intrapulmonary artery pseudoaneurysm is a rare but potentially life-threatening complication that can lead to massive hemoptysis, most commonly seen in the context of chronic pulmonary tuberculosis. Endovascular embolization is the preferred treatment modality in indicated cases. However, in certain peripheral lesions that are difficult to access or when endovascular intervention fails, direct puncture of the pseudoaneurysm under computed tomography guidance can be an effective alternative. We report a case of a tuberculosis-related pulmonary artery pseudoaneurysm that failed endovascular embolization and was successfully treated by percutaneous direct puncture under computed tomography scan guidance using NBCA glue. This case highlights the role of percutaneous access in managing complex pseudoaneurysms that are not amenable to conventional techniques.
Keywords: Pulmonary artery pseudoaneurysm; Intrapulmonary pseudoaneurysm; Peripheral pulmonary pseudoaneurysm embolization; Percutaneous embolization.
Citation: Loc Tran Q, Cong Cung V, Luong Hoang V, Tam Tran N, Cuong Vu M, et al. Percutaneous treatment of pulmonary artery pseudoaneurysm embolization after failed endovascular access a case report and literature review. SciBase Cardiol. 2025; 3(1): 1018.
Introduction
Intrapulmonary Pseudoaneurysm (IPP) is a rare vascular abnormality with potentially life-threatening consequences. It most commonly presents with hemoptysis, which can be massive if the pseudoaneurysm ruptures, with a reported mortality rate of up to 50%. IPPs can be spontaneous or secondary to various causes such as trauma, infection (particularly pulmonary tuberculosis), pulmonary tumors, vasculitis, or pulmonary artery hypertension. Studies have documented IPPs in approximately 11% of patients undergoing bronchial artery angiography for hemoptysis and in up to 14% of patients with chronic pulmonary tuberculosis [1,2].
Currently, Computed Tomography (CT) is the primary imaging modality for detecting intrapulmonary artery pseudoaneurysms. In certain cases, the pseudoaneurysm may be better visualized on systemic angiography (including bronchial and non-bronchial systemic arteries) due to the phenomenon of retrograde flow within the pulmonary arterial branches at the lesion site [1,2].
Management options include medical therapy, surgery, and endovascular intervention. Interventional treatment usually begins with embolization of the systemic arterial branches. However, if hemoptysis remains uncontrolled, selective pulmonary artery access and targeted embolization of the pseudoaneurysm may be necessary. Even after successful occlusion, hemoptysis may recur but often responds well to subsequent embolization of systemic arteries [1,2].
In complex cases—such as small feeding arteries, aberrant vascular anatomy, or failure of vascular access—where surgery is not feasible, direct puncture of the pseudoaneurysm under imaging guidance (DSA or CT) can be an effective alternative. Although this technique can achieve successful results, it carries risks of serious complications, including pneumothorax, pseudoaneurysm rupture, or non-target embolization [3].
This report presents a case of a tuberculosis-related pulmonary artery pseudoaneurysm that was successfully treated with percutaneous direct puncture under CT guidance after endovascular approaches failed. The discussion highlights the role, efficacy, and indications for this technique based on current literature.
Clinical case
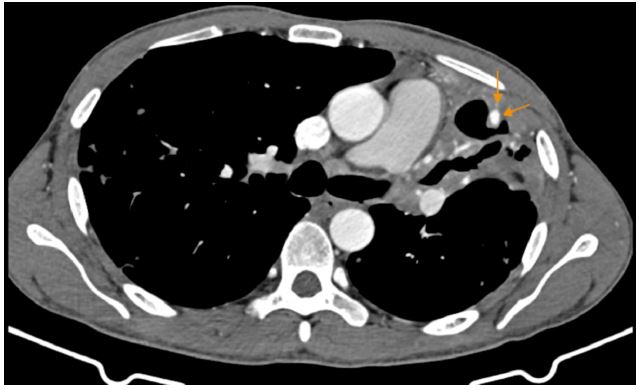
A 39-year-old male with a history of discontinued pulmonary tuberculosis treatment one year prior was admitted for hemoptysis. A few days before admission, he experienced intermittent episodes of hemoptysis, with the most significant bleeding estimated at 30-50 mL. No treatment had been initiated at that time. Chest Computed Tomography (CT) revealed a cavitary consolidation in the left upper lobe, with a 5 × 4 mm pseudoaneurysm located at the peripheral wall of the cavity. There was also evidence of a dilated left bronchial artery and hypertrophied intercostal and subclavian artery branches.
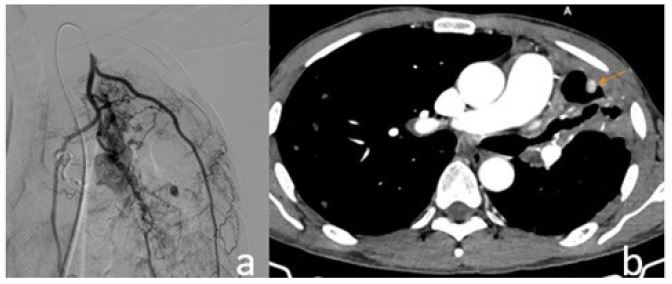
The patient initially underwent endovascular embolization. Selective angiography of the left internal mammary artery identified the pseudoaneurysm, which was embolized using NBCA glue mixed with lipiodol at a 1:4 ratio. Despite this, the patient continued to experience mild, intermittent hemoptysis. Follow-up CT imaging showed complete occlusion of the left bronchial artery and collateral branches from the left subclavian artery, but the pseudoaneurysm persisted with reduced contrast enhancement.
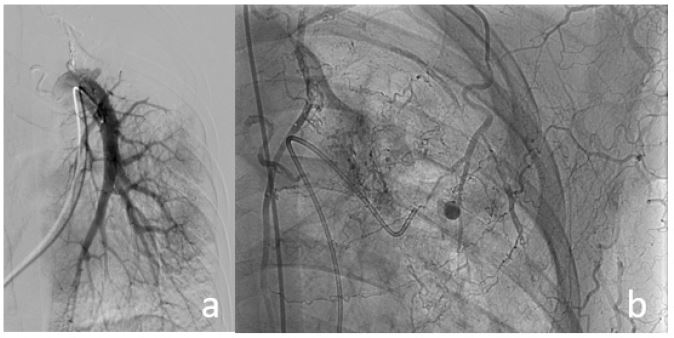
A second intervention was planned. Attempts to access the pseudoaneurysm via the pulmonary artery failed due to the small and peripheral feeding branch. Delayed-phase (7-second) angiography of the left subclavian artery revealed ongoing perfusion of the pseudoaneurysm through a lateral thoracic artery branch. An attempt at direct puncture under DSA guidance with an 18G needle was unsuccessful, and the patient experienced a 50 mL hemoptysis episode, which was managed locally. This confirmed that the pseudoaneurysm still had active blood flow.
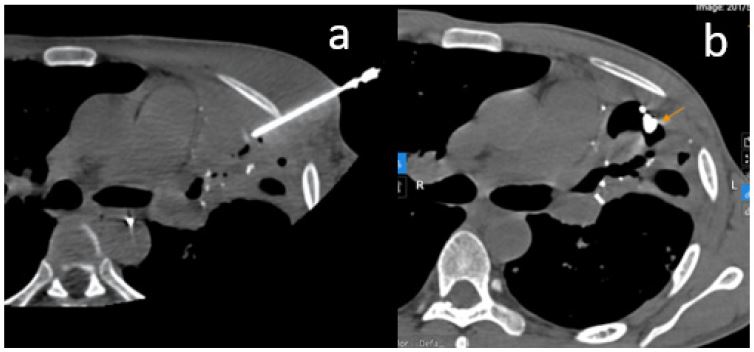
Subsequently, the patient was referred for CT-guided percutaneous intervention. Under CT guidance, an 18G needle was advanced into the pseudoaneurysm, and contrast injection verified intraluminal positioning. Embolization was performed with NBCA: lipiodol at a 1:2 ratio. Post-procedural contrast-enhanced CT demonstrated complete filling of the pseudoaneurysm sac with glue, indicating successful occlusion. The patient experienced no further hemoptysis and was discharged after 4 days, with initiation of standard anti-tuberculosis therapy.
This case underscores that while endovascular embolization remains the first-line treatment for pseudoaneurysms—thanks to its advantages in dynamic flow assessment and controlled delivery—percutaneous direct puncture should be considered a salvage option when vascular access fails or surgery is contraindicated. However, this technique carries risks such as hemoptysis, pneumothorax, and non-target embolization, and requires cautious execution.
Discussion
Was the pseudoaneurysm observed in the above clinical case truly a Pulmonary Artery Pseudoaneurysm (PAP)? The absence of a pseudoaneurysm on DSA of the left pulmonary artery does not entirely exclude its presence, especially given its peripheral location and small size. The affected branches exhibited wall damage, anatomical complexity, and altered flow dynamics, which hindered successful selective catheterization. Upon successful direct puncture of the pseudoaneurysm, NBCA glue was observed to pool in a focal area and reflux into a small pulmonary arterial branch, indicating retrograde flow and confirming communication with the pulmonary circulation.
Pulmonary Artery Pseudoaneurysm (PAP) due to tuberculosis is a rare but particularly dangerous vascular complication, typically seen in cases of active or chronic pulmonary tuberculosis. This condition was first described by Fritz Valdemar Rasmussen in 1868, who reported pseudoaneurysm formation resulting from erosion of the pulmonary artery wall adjacent to a tuberculous cavity. This process leads to progressive vessel wall thinning and the development of a blood-filled sac. Unlike true aneurysms, pseudoaneurysms lack the tunica media and adventitia, making them more prone to rupture and causing life-threatening massive hemoptysis [1,4].
In our patient, there was a history of tuberculosis treatment that had been discontinued for the past year. The pseudoaneurysm was located near a residual tuberculous cavity in the left upper lobe and was supplied by both bronchial and non-bronchial systemic arteries—features consistent with the typical characteristics of post-tuberculosis pulmonary artery pseudoaneurysms.
Intrapulmonary pseudoaneurysms are typically identified using Multidetector Computed Tomography (MDCT) angiography. The detection rate among patients with hemoptysis undergoing angiographic imaging ranges from 5-11%. Often, these lesions are identified retrospectively or on follow-up scans. The use of Multiplanar Reconstructions (MPR), especially in coronal and axial planes, can enhance detection sensitivity. Misdiagnosing a pulmonary pseudoaneurysm can delay appropriate treatment and lead to unnecessary interventions such as biopsy or surgery, due to confusion with endobronchial lesions or pulmonary tumors [1,5].
In our case, the patient underwent contrast-enhanced 64-slice chest CT with multiplanar reconstructions. Imaging revealed a cavitary consolidation in the left upper lobe, with a 5 × 4 mm pseudoaneurysm located in the cavity wall, along with dilation and hypertrophy of the left bronchial artery, intercostal branches, and the left subclavian artery. This underscores the vital role of CT imaging in evaluating patients with hemoptysis, particularly for identifying pulmonary vascular lesions.
Bronchial artery aneurysms and pseudoaneurysms are rare, with only a limited number of cases reported, yet they can cause life-threatening hemoptysis if ruptured—due to the high-pressure systemic arterial supply from the thoracic aorta. Although less common, bronchial artery pseudoaneurysms still demand prompt treatment—even when asymptomatic—because rupture risk is unpredictable and does not necessarily correlate with lesion size. Currently, endovascular embolization is the preferred treatment, owing to its effectiveness and minimally invasive approach, using various embolic agents such as coils, gelatin, or NBCA glue [3].
In this clinical case, the pseudoaneurysm was associated with a residual tuberculous cavity and supplied by both bronchial and non-bronchial systemic arteries—features typical of tuberculous-related intrapulmonary pseudoaneurysms. The initial management involved embolization of systemic branches via the left internal mammary artery with NBCA glue, which resulted in a partial, but not complete, occlusion. The pseudoaneurysm persisted, although with reduced contrast enhancement. This scenario highlights the limitations of isolated systemic embolization in complex cases, especially when target vessels are small and difficult to access.
In situations where endovascular access fails or is anatomically unfeasible, percutaneous puncture techniques may be considered, although they carry inherent risks such as pneumothorax or pseudoaneurysm rupture if not performed with precision [3,6]. In the reported case, the initial attempt at direct puncture under DSA guidance failed and resulted in a temporary recurrence of hemoptysis. Subsequently, CT-guided intervention allowed for precise localization of the pseudoaneurysm and accurate delivery of glue, achieving definitive therapeutic success. Using a higher NBCA-to-lipiodol ratio (1:2) increased the mixture’s viscosity, limiting glue dispersion and reducing the risk of non-target embolization.
The successful outcome in this case further supports the potential role of direct percutaneous pseudoaneurysm puncture as a salvage technique when standard endovascular approaches fail. However, it should be regarded as a last-resort option, reserved for institutions equipped with appropriate imaging modalities, technical expertise, and the capacity to manage complications. Proper selection of glue concentration and volume, accurate needle placement, and close post-procedural monitoring are critical to maximize treatment efficacy and minimize risks.
Conclusion
Intrapulmonary artery pseudoaneurysm is a rare but potentially life-threatening complication, especially in the context of chronic pulmonary tuberculosis. Embolization via both systemic and pulmonary arterial routes remains the first-line treatment because of its proven efficacy, minimally invasive nature, and better control over embolic materials. However, in cases where these approaches are unsuccessful due to unfavorable anatomy or peripheral, inaccessible lesions, direct percutaneous puncture under imaging guidance—particularly CT—can serve as an effective alternative, especially when surgical options are limited.
References
- Chen Y, Gilman MD, Humphrey KL, et al. Pulmonary artery pseudoaneurysms: clinical features and CT findings. Am J Roentgenol. 2017; 208: 84-91.
- Sbano H, Mitchell AW, Ind PW, et al. Peripheral pulmonary artery pseudoaneurysms and massive hemoptysis. Am J Roentgenol. 2005; 184: 1253-1259.
- Patton A, Hylands A, Jogi RM. Navigating complexity and sealing the threat: ultrasound and CT guided percutaneous glue embolization of bronchial artery pseudoaneurysm with challenging anatomy. Radiol Case Rep. 2025; 20: 454-459.
- Pallangyo P, Lyimo F, Bhalia S, et al. Bilateral multiple pulmonary artery aneurysms associated with cavitary pulmonary tuberculosis: a case report. J Med Case Rep. 2017; 11: 196.
- Nguyen ET, Silva CIS, Seely JM, et al. Pulmonary artery aneurysms and pseudoaneurysms in adults: findings at CT and radiography. Am J Roentgenol. 2007; 188: W126-W134.s
- Urlings TAJ, Irani FG, Velaga J, et al. Ultrasound- and fluoroscopic-guided embolization of a bronchial artery pseudoaneurysm in a patient with lung cancer. J Vasc Interv Radiol. 2017; 28: 1323-1325.