
SciBase Journals
SciBase Clinical and Medical Case Reports
ISSN 2995-5874
- Article Type: Case Report
- Volume 2, Issue 3
- Received: Jul 08, 2024
- Accepted: Aug 22, 2024
- Published Online: Aug 29, 2024
From Allergies to ATAK: A Complex Case Report Following Ciprofloxacin Administration
Soorampally Vijay1,3; Bharath Raj Kidambi2*; Sriram Veeraraghavan2
1Department of Cardiology, Trinity Hospital, Bangalore, India.
2Department of Cardiology, SRM Medical College and Research Centre, Potheri, Chengalpattu, Tamil Nadu - 603203, India.
3Specialist Cardiologist, Department of Cardiology, Al Dhannah Hospital, Ruwais, Abu Dhabi, UAE.
*Corresponding Author: Bharath Raj Kidambi
Department of Cardiology, SRM Medical College and
Research Centre, Potheri, Chengalpattu, Tamil Nadu -
603203, India.
Tel: +971-551384611;
Email: drbkid@gmail.com
Abstract
This case report describes a complex clinical scenario involving a previously healthy middle-aged woman who received ciprofloxacin for acute otitis media and subsequently developed symptoms of allergic hypersensitivity and anaphylaxis. Following an intramuscular adrenaline injection for anaphylaxis, she experienced chest pain consistent with Inferior Wall Myocardial Infarction (IWMI), with discordant echocardiography findings and normal epicardial coronary arteries on coronary angiography. The case is the intricate interplay of the ATAK (Adrenaline, Takotsubo, Anaphylaxis, Kounis) complex, with implications for diagnosis and management.
Keywords: ATAK; Kounis syndrome; Allergic Myocardial infarction; Anaphylaxis.
Citation: Vijay S, Kidambi BR, Veeraraghavan S. From Allergies to ATAK: A Complex Case Report Following Ciprofloxacin Administration. SciBase Clin Med Case Rep. 2024; 2(3): 1028.
Case presentation
Introduction: Acute otitis media is commonly treated with antibiotics such as ciprofloxacin. However, adverse reactions, including allergic hypersensitivity leading to anaphylaxis, can occur. The ATAK complex, encompassing adrenaline-induced Takotsubo syndrome, anaphylaxis, and Kounis syndrome, represents a diagnostic challenge and is difficult to manage in clinical practice.
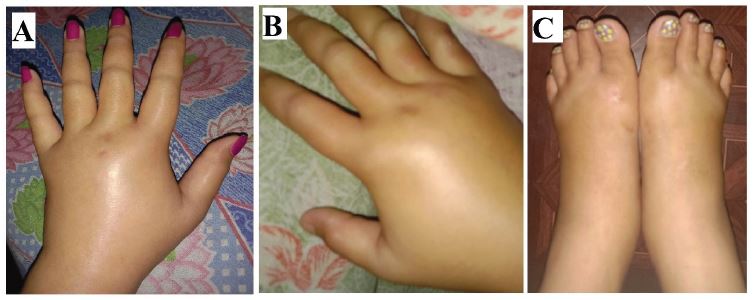
Patient presentation: A 35-year-old woman, without any prior co-morbidities, presented to the emergency department with symptoms of generalized itching and swelling of both hands and feet, which started 2 hours after the intake of ciprofloxacin for acute otitis media. There was no known history of allergy to any drugs or atopy in the past. On initial examination, her blood pressure was 132/84 mm of Hg; pulse rate was 96 per minute, and a new onset of swelling on the hands and feet (Figure 1).
Systemic examination revealed a bilateral wheeze, with progressive worsening breathlessness. Considering impending anaphylaxis, 0.5 mg of adrenaline 1:1000 dilution was given. A few minutes after administration of adrenaline, she complained of severe retrosternal chest pain [12] lead ECG was obtained (Figure 2). She developed hypotension with the blood pressure of 90/60 mmHg.
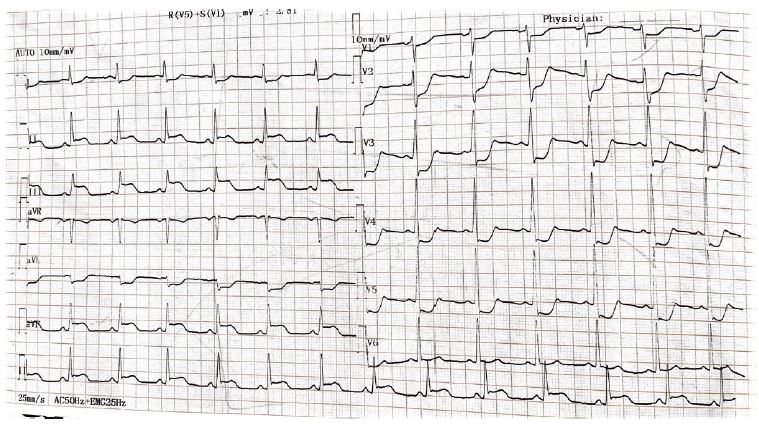
Clinical course: The patient was being stabilized with an Intravenous fluid bolus of normal saline, and was being prepared for catheterization lab. The ECG was suggestive of inferior Wall Myocardial infarction due to probable RCA occlusion (ST elevation in lead III, II, and avF, ST depression in I, aVL, and V1-V5). However, a quick echocardiogram revealed apical ballooning Due to moderate hypokinesia of the mid to distal septum, apical septum, apex, and apicolateral segments with a reduced ejection fraction of 35% (Supplementary video 1).
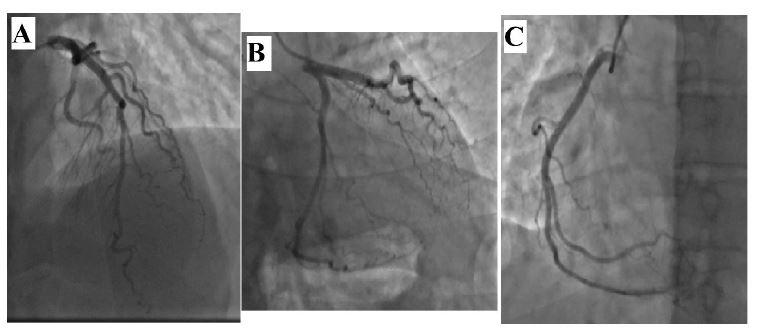
As this did not correlate with the infarct-related territory on ECG, she was shifted urgently to the catheterization lab which revealed normal epicardial coronaries (Figure 3).
Anaphylaxis: IM adrenaline 0.5 mg (1:1000 dilution) was given initially, later started on IV diphenhydramine 50 mg twice daily, and IV ranitidine Twice daily. She was started on oral prednisolone at 40 mg once daily with a plan to taper on follow-up.
Inferior wall MI (Type I Kounis): She received loading doses of aspirin 150 mg, ticagrelor 90 mg, and atorvastatin 80 mg before angiography. After the angiography atorvastatin 80 mg was continued and DAPT was discontinued. Oral diltiazem was started to treat coronary vasospasm.
Takotsubo cardiomyopathy: There was a dilemma in starting an ACE inhibitor or beta blocker for the low EF, due to fear of exacerbation of angioedema and coronary vasospasm.
Avoidance of allergen triggers: Extensive medication reconciliation was done and patient education was provided for avoidance of known allergens, especially antibiotics. She was referred to an Allergen specialist for further evaluation and management.
Follow-up: The patient was stabilized in the ICU, and discharged 3 days later with atorvastatin 80 mg, diltiazem 60 mg, prednisolone 40 mg (with a plan to taper every week), levocetirizine 5 mg. 1 week later she was started on medications for her LV dysfunction - carvedilol 3.125 mg, and valsartan 80 mg due to their low chances of coronary vasospasm and angioedema. She tolerated these tablets well and at 3 months follow-up, there was complete resolution of LV dysfunction.
Labs
| Test | Result | Normal range |
|---|---|---|
| Complete Blood Count (CBC) | ||
| White Blood Cell Count (WBC) | 14,000 cells/μL | 4,000-11,000 cells/μL |
| Eosinophil Count | 754 cells/μL | 0-450 cells/μL |
| Serum cardiac biomarkers | ||
| Troponin | Initial: 0.14 ng/mL | 0-0.04 ng/mL |
| After angiography: 2.5 ng/mL | ||
| Creatine Kinase-MB (CK-MB) | 36 U/L | 0-25 U/L |
| Electrolyte panel | ||
| Potassium (K+) | 4.8 mmol/L | 3.5-5.0 mmol/L |
| Calcium (Ca2+) | 9.3 mg/dL | 8.5-10.5 mg/dL |
| Magnesium (Mg2+) | 2.2 mg/dL | 1.7-2.2 mg/dL |
| Liver Function Tests (LFTs) | ||
| Alanine Aminotransferase (ALT) | 21 U/L | 0-40 U/L |
| Aspartate Aminotransferase (AST) | 25 U/L | 0-35 U/L |
| Alkaline Phosphatase (ALP) | 78 U/L | 40-130 U/L |
| Total Bilirubin | 0.8 mg/dL | 0.3-1.0 mg/dL |
| Renal Function Tests (RFTs) | ||
| Blood Urea Nitrogen (BUN) | 15 mg/dL | 7-20 mg/dL |
| Creatinine | 0.9 mg/dL | 0.6-1.1 mg/dL |
| Coagulation Profile | ||
| Prothrombin Time (PT) | 12 seconds | 10-13 seconds |
| International Normalized Ratio (INR) | 1.0 | 0.8-1.2 |
| Activated Partial Thromboplastin Time (aPTT) | 30 seconds | 25-35 seconds |
| Other Tests | ||
| Serum Tryptase | 25 ng/mL | 2-15 ng/mL |
| Serum Chymase | 30 ng/mL | 5-15 ng/mL |
Diagnosis
Timeline of events:
0 Hours: Received ciprofloxacin for acute otitis media.
2 hours: Onset of allergic hypersensitivity symptoms.
2 hours 30 minutes: Intramuscular adrenaline injection for suspected anaphylaxis.
2 hours 40 minutes: (Shortly after adrenaline injection): Development of chest pain and ECG changes suggestive of IWMI.
2 hours 45 minutes: Takotsubo cardiomyopathy noted in Echocardiography.
3 hours: Coronary angiography - normal epicardial coronaries.
Based on the clinical presentation, ECG findings, laboratory investigations, and echocardiography demonstrating apical ballooning, the patient was diagnosed with ciprofloxacin-induced anaphylaxis, Kounis syndrome type I (Coronary vasospasm), Adrenaline associated Takotsubo consistent with the ATAK complex [1].
| Aspect | Standard acute MI management | Kounis syndrome management |
|---|---|---|
| Trigger | Atherosclerotic plaque rupture or thrombosis | Allergic reaction or hypersensitivity trigger |
| Initial treatment | Immediate reperfusion therapy (e.g., PCI, thrombolysis) | Treatment of anaphylaxis (e.g., adrenaline, antihistamines, corticosteroids) |
| Antiplatelet therapy | Aspirin, P2Y12 inhibitors (e.g., clopidogrel, ticagrelor) | May be used cautiously due to the increased risk of bleeding in anaphylaxis |
| Anticoagulation therapy | Heparin, low molecular weight heparin | May be used cautiously due to the increased risk of bleeding in anaphylaxis |
| Beta-blockers | Recommended for secondary prevention | May be used cautiously due to potential exacerbation of bronchospasm, coronary vasospasm |
| Coronary angiography | Essential for diagnosis and management | May be deferred in certain cases to avoid exacerbating anaphylaxis |
| Allergen avoidance | N/A | Essential to prevent future allergic reactions |
| Long-term management | Secondary prevention strategies (e.g., statins, ACE in- hibitors, beta-blockers) | Focus on allergen avoidance and management of allergic reactions along with OMT for HF. |
Discussion
Drug-induced anaphylaxis is commonly seen with penicillin, NSAIDs, sulphonamides, and antibiotics. Anaphylaxis has been reported with the first-ever dose of fluoroquinolones without the need for sensitization [2,3]. Adrenaline is the drug of choice for anaphylaxis, but it has been shown in some reports to precipitate cardiac events due to its metabisulphite component in certain preparations [4,5]. The catecholamine surge along with inflammatory mediators of anaphylaxis play a central role in orchestrating Kounis syndrome and stress-induced cardiomyopathy. Antibiotics, notably ciprofloxacin in our case, are one of the most common triggers of Kounis syndrome, with approximately 70% of cases occurring within 30 minutes post-administration. Type I Kounis syndrome, accounting for 72.6% of cases, is primarily characterized by coronary artery spasms triggered by the release of inflammatory mediators, which may or may not be accompanied by an elevation in cardiac enzymes. Type II occurs in individuals with underlying atheromatous disease; here, the inflammatory mediators can induce a coronary vasospasm and potentially lead to the rupture of atheromatous plaques, culminating in an acute myocardial infarction. Type III is associated with patients who have a coronary artery stent in place, where inflammatory mediators can cause stent thrombosis. It’s important to note that coronary artery spasm is typically a hyperacute condition [6,7].
Additionally in our patient, symptoms encompassing chest pain, following adrenaline administration with features suggestive of Takotsubo cardiomyopathy on Echocardiography are consistent with previous literature on ATAK complex [8,9]. During extreme stress, elevated catecholamines, along with exogenously administered epinephrine, can trigger a negative inotropic effect on the heart via β-adrenoceptors, potentially due to biased agonism leading to phosphorylation and signaling disruption. This surge can cause reversible myocardial stunning, notably in the apical and midventricular regions, a hallmark of Takotsubo Syndrome (TTS). Our case aligns closely with the documented clinical manifestations of the ATAK complex [10].
Management challenges: There are no specified guidelines for managing ATAK complex, and treatment has been individualized based on a few case reports. Managing patients with the ATAK complex requires a multidisciplinary approach, encompassing allergists, cardiologists, and emergency physicians. Treatment strategies may include addressing allergic reactions, managing Takotsubo syndrome, and mitigating coronary vasospasm. It differs from conventional management of STEMI in the following way [11,12].
Conclusion
This case highlights the diagnostic and therapeutic issues associated with the ATAK complex, stressing the significance of appropriate diagnoses and managing the complex interplay between adrenaline, Takotsubo syndrome, anaphylaxis, and Kounis syndrome. A full understanding of these illnesses and their possible interactions is required for the best patient care and outcomes.
Disclosure statement: The authors report no financial relationships or conflicts of interest regarding the content herein.
References
- Margonato D, Abete R, Di Giovine G, Delfino P, Grillo M, et al. Takotsubo cardiomyopathy associated with Kounis syndrome: A clinical case of the ATAK complex. J Cardiol Cases. 2019; 2(2): 52-6. https://doi.org/10.1016/J.JCCASE.2019.03.007.
- Dhopeshwarkar N, Sheikh A, Doan R, Topaz M, Bates DW, et al. Drug-Induced Anaphylaxis Documented in Electronic Health Records. J Allergy Clin Immunol Pract. 2019; 1(1): 103-11. https://doi.org/10.1016/j.jaip.2018.06.010.
- Navarro-Navajas A, Casallas I, Isaza D, Ortiz P, Baracaldo-Santamaría D, et al. Type III Kounis Syndrome Secondary to CiprofloxCiprofloxacin-Induced Hypersensitivity. Medicina (B Aires). 2022; 58(7). https://doi.org/10.3390/medicina58070855
- Borchert T, Hübscher D, Guessoum CI, Lam TDD, Ghadri JR, et al. Catecholamine-Dependent β-Adrenergic Signaling in a Pluripotent Stem Cell Model of Takotsubo Cardiomyopathy. J Am Coll Cardiol. 2017; 70(8): 975-91.
- Ballesteros RV, Carlos Gómez J, Olmos C, Vilacosta I. Case Report Kounis and Takotsubo, Two Syndromes Bound by Adrenaline: The ATAK Complex. 2023. https://doi.org/10.1155/2023/7706104.
- Renda F, Landoni G, Trotta F, Piras D, Finco G, et al. Kounis Syndrome: An analysis of spontaneous reports from international pharmacovigilance database. Int J Cardiol. 2016; 203: 217-20.
- Kounis NG, Koniari I, Velissaris D, Tzanis G, Hahalis G. Kounis syndrome-not a single-organ arterial disorder but a multisystem and multidisciplinary disease. Balkan Med J. 2019; 36(4): 212-21.
- Margonato D, Abete R, Di Giovine G, Delfino P, Grillo M, et al. Takotsubo cardiomyopathy associated with Kounis syndrome: A clinical case of the ATAK complex. J Cardiol Cases. 2019; 20 2(2): 52-6. https://doi.org/10.1016/J.JCCASE.2019.03.007.
- Minciullo PL, Amato G, Vita F, Pioggia G, Gangemi S. ATAK Complex (Adrenaline, Takotsubo, Anaphylaxis, and Kounis Hypersensitivity-Associated Coronary Syndrome) after COVID-19 Vaccination and Review of the Literature. Vaccines (Basel). 2023; 11(2). https://doi.org/10.3390/vaccines11020322.
- Lyon A. Stress in a Dish: Exploring the Mechanisms of Takotsubo Syndrome. J Am Coll Cardiol. 2017; 70(8): 992-5.
- Lyon AR, Bossone E, Schneider B, Sechtem U, Citro R, et al. Current state of knowledge on Takotsubo syndrome: a Position Statement from the Taskforce on Takotsubo Syndrome of the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail. 2016; 18(1): 8-27. Available from: https://doi.org/10.1002/ejhf.424.
- Badami KG. Transfusion double whammy? Adrenaline‐takotsubo‐anaphylaxis‐Kounis complex post transfusion? Vox Sang. 2022; 117(6): 862-5. https://doi.org/10.1111/vox.13257.