
SciBase Journals
SciBase Clinical and Medical Case Reports
ISSN 2995-5874
- Article Type: Case Report
- Volume 2, Issue 4 - 2024
- Received: Jul 22, 2024
- Accepted: Sep 11, 2024
- Published Online: Sep 18, 2024
Effects of Stress-Induced Neuroendocrine-Immune Interaction on Periodontium: A Review
Surajit Mistry*; Debarati Bhowmick; Indrasri Das; Argha Rudra
Department of Periodontics, Dr. R. Ahmed Dental College and Hospital, 114, A.J.C. Bose Road, Kolkata, West Bengal, Pin- 700014, India.
*Corresponding Author: Surajit Mistry
Department of Periodontics, Dr. R. Ahmed Dental College and Hospital, 114, A.J.C. Bose Road, Kolkata, West Bengal, Pin- 700014, India.
Email: dr.surajitmistry@rediffmail.com
Abstract
This review discusses recent advances in our understanding of the relationships between psychological stress, neuroendocrine- immune system, and periodontitis, including how host stress responses affect immune function, alter the oral microbiome and biofilm formation, and promote disease progression. Stress is well known to be a modifiable risk factor in a variety of chronic diseases, including chronic periodontitis, in which the host stress response not only alters immune function but also causes dysbiosis of oral biofilm by expressing more pathogenic genes and taxa composition, which acts via several neuroendocrine mechanisms. As a result, it influences the development and progression of periodontal disease. However, the difficulty in measuring stress in terms of amount and duration in patients is a significant hurdle to addressing the negative impact of stress on periodontal health.
Keywords: Psychological stress; Modifiable risk factor; Biofilm; Neuroendocrine; Chronic periodontitis.
Citation: Mistry S, Bhowmick D, Das I, Rudra A. Effects of Stress-Induced Neuroendocrine-Immune Interaction on Periodontium: A Review. SciBase Clin Med Case Rep. 2024; 2(4): 1030.
Introduction
The effort to understand the molecular mechanisms underlying psychosocial stress, oral inflammatory diseases (such as periodontal/peri-implant diseases), and wound healing has steadily increased since the 1970s, when a link between stress and oral disease was discovered [1]. Recent studies have discovered a stronger connection between long-term psychological stress and disorders and diseases of the periodontium and periosteum because of immunological alterations, oral microbiome dysbiosis, collagen turnover ratios, and the emergence of systemic and regional diseases [1,2]. Stress and depression worsen life quality and productivity at work, increase the risk of developing chronic illnesses, and raise the financial burden of medical expenses [3,4]. According to a survey, healthcare costs for employees with depression are 48% more than those who are not at risk [3].
Stress is a transactional process that occurs when an event is considered as important to an individual’s well-being, has the potential for harm or loss, and necessitates psychological, physiological, and/or behavioral responses to manage the event and its consequences [5]. Stress can simply be described as tight or strained [6]. Recently World health organization defined stress as a state of worry or mental tension caused by a difficult situation [8]. It is a protective human response that drives us to confront problems and threats in our lives. Everyone experiences stress to some degree. Stress is the brain’s reaction to promote activities that protect organisms from danger, but it develops when people’s coping abilities alter to adjust or tolerate actual or perceived threat [9,10]. To put it succinctly, it refers to an individual’s capacity to manage stressors, which are defined as any circumstance, impact, or state that causes mental or bodily strain [10]. Stressors can be internal or external influences that necessitate changes or coping methods on the part of the afflicted person. It is determined by the interaction between a person’s internal makeup and external environment. For example, a person with solid social support and positive relationships has higher coping abilities than those who have had terrible childhood experiences, making the former more resilient than the latter.
Stress has been shown to induce or worsen inflammation, acting as a predisposing factor in the pathogenesis of many chronic diseases such as cardiovascular, metabolic, digestive, pulmonary, and rheumatologic diseases, as well as infectious, allergy, autoimmune, or neoplastic etiologies, and periodontitis [4,10]. Stress is found to be connected with respiratory disorders in a dose-dependent manner [11]. There are several modifiable risk factors that contribute to periodontal disease, such as diabetes and smoking [12]. However, the study recognizes the link between a stressed lifestyle and poor dental hygiene [12,13]. Stress has long been recognized as a risk factor in the pathogenesis of necrotizing ulcerative gingivitis, and chronic/aggressive periodontitis [10,12,14]. Moreover, clinical attachment loss was more with stressed individuals [15]. Therefore, in this review article we are highlighting the influence of psychosocial stress in the health of periodontium.
Stress: Clinical features and types
Stress is an umbrella term for events in which the environmental demands of a situation overwhelm an individual’s perceived psychological and physiological ability to cope with them effectively [16,17]. It can appear in a variety of ways, including inability to concentrate, intractable headaches, bodily pain, and disorders. Furthermore, it is known to exacerbate the progression of underlying chronic illnesses and increase substance abuse, such as smoking and alcohol consumption [8]. In addition, it causes neglected oral health, increases in plaque, and gingival inflammation [18]. Stress can be acute or chronic, based on the duration [19]. Acute stress lasts for a brief period, such as engaging in preparing for tests, public talk, being overburdened with work, and meeting a deadline, whereas chronic stress lasts for a long period of time, such as dealing with limited resources, relationship issues, or long-term health problems. The harmful effects of acute stress in periodontium are not well documented. Chronic stress, on the other hand, has a variety of detrimental effects on the body and works via complex neuroendocrine mechanisms, as demonstrated below [19].
Stress and biologic response of body
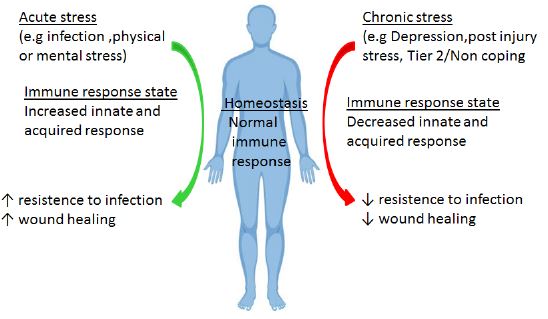
The physiologic stress response is an evolutionarily conserved physiological mechanism that connects an organism to its surroundings. Stressor cues can be physical or psychological in nature. Physical cues that activate stress include trauma, infection, or tumor. Psychologic or emotional cues may come from life events like financial difficulties, caregiving, or the loss of a spouse; or post-traumatic stress /depression (Figure 1). Acute stressors (infection, surgery) often present with upregulation of innate immune mechanisms but suppression of cellular immunity.
Conversely, chronic stress frequently manifests as a reduction of innate and cellular immune responses [20]. In their evolutionary origins, the stressors of the acute fight-or-flight scenarios induce positive adaptations that enable the body to recover from injury fast. For instance, following acute trauma experienced in periodontal surgery, the innate mechanism is heightened to promote debris removal and healing of wounds. On the other hand, the immune system is adversely affected in chronic stress to a greater extent depending on how much these stressors deviate from these biologically conserved norms [20]. For example, during periodontal surgery under chronic stress, there may be a reduced debris clearance response, which delays wound healing and generates a less favorable regeneration milieu. The precise point at which stressors shift from acute to chronic is currently an issue of intense discussion. However, the main processes that cause these systemic changes include the Hypothalamic-Pituitary-Adrenal (HPA) axis, which produces glucocorticoids, and the adrenergic nerve signaling axis, which produces norepinephrine, adenosine triphosphate, and neuropeptide Y. The hypothalamic-pituitary-adrenal axis and sympathetic nervous system both release a variety of different chemicals during the stress response cascade, but an in-depth discussion of these additional chemokines is beyond the scope of this paper.
Stress and neuroendocrine system
Stress and its influence on HPA axis
Central nervous system interacts with both immune and endocrine system [4]. Certain stress mediators including monoamines, neuropeptides and steroid hormones sends signal to CNS and assists in adaptation and survival via autonomic, endocrine, metabolic and immune responses while chronic stress on the other hand cause dysregulation of these pathways that causes detrimental effects [4]. The Hypothalamic-Pituitary-Adrenocortical Axis (HPA) and sympathetic-adrenal-medullary are two major pathways [4,10,11]. The paraventicular nucleus of hypothalamus is activated during acute stress and releases arginine vasopressin and Corticotrophin Releasing Hormones (CRH) which further stimulates pituitary to release Adrenocorticotrophic Hormone (ACTH) that stimulates adrenal medulla to secrete cortisol [4,10]. Moreover, epinephrine is released via activation of noradregenic centre in the locus correleus of brainstem and medulla of adrenal gland. The sudden cortisol rise just after acute stress like divorce or accident increases circulating inflammatory cytokines but in chronic stress although the circulating level of cortisol is high but it does not able to modulate the inflammatory response due to glucocorticoid receptor resistance [4,10]. Persistent dysregulation of HPA is documented in many chronic illness-like autoimmune diseases, cardiovascular diseases, upper respiratory tract infection, periodontitis etc [4,10]. Furthermore, Regulatory T cells which are known suppress inflammatory cascade by producing Transforming growth factor-beta1 and Interleukin (IL-10) and suppresses CD4+ and CD8+ effector cell responses are reduced in stress [4,10]. A diminished T regs is implicated in patients with atherosclerosis that harbors P. Gingivalis [10,21]. Similarly, inflammation is one of the pivotal connecting links between stress and periodontal disease [4,10]. With chronic stress, the number of circulating neutrophils and the ratio of Th-1 and Th-2 cells are drastically reduced thereby impairing the proliferation of T cells and subsequent antibody response.. Besides that, chronic stress as they cause glucocorticoid receptor resistance they jeopardize the immunosuppressive action of cortisol on lymphocytes. A metanalaysis studies proves that blood levels of IL-6, TNF-alpha, IL-1beta and C-reactive proteins are elevated with stress response [10,22]. The proinflammatory mediators are generally elevated in gingival crevicular fluids in chronic periodontitis which draws an plausible explanation of influence of chronic stress and pathogenesis of periodontal disease [10,23].
Stress and its influence on adrenergic signaling axis
The adrenergic nerve signaling cascade molecules (norepinephrine) directly affect the vasculature in the periodontium results in limited cellular and nutrient diffusion, causing poor adaptive immune responses and restricting repair reactions in periodontal and periosteal (bone) tissues [24]. Adrenergic nerve stimulation also limit vascular perfusion at lymphoid tissues, resulting in immune dysregulation, especially those noted in marginal alveolar bone loss and periodontal disease progression.
Neurologic alterations affecting behavior
Stress duration can also start physically adaptive changes in cognition and behaviour, such as feeding/hunger, vigilance, and alertness, in addition to these intrinsic peripheral and central system responses. In reality, research using functional imaging has demonstrated that psychosocial stress and illnesses associated to it can cause morphologic alterations in the brain, particularly in the hippocampus [25].
Psychobiologic effects on oral structures and wound healing capacity
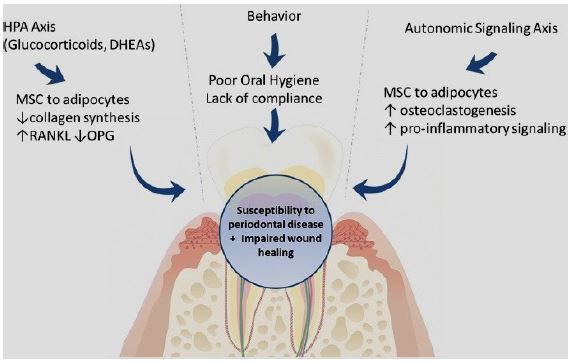
Both physical and psychologic stimuli can affect a biologic system at an organ system level, cellular level, and molecular level through mechanisms of the hypothalamic-pituitary-adrenal axis, adrenergic nerve signaling axis, and behavior modification (Figure 2). Periodontal structures, including the mucosal tissues/keratinocytes/periodontal extracellular matrix, periosteum/bony tissue, and the microbiologic/periodontal microenvironment, are most susceptible to stress-related dysbiosis. Oral soft tissue wound healing follows a well-established trajectory that consists of four categories: (1) hemostasis/inflammation; (2) migration; (3) proliferation; and (4) remodeling [26]. It appears that the psychobiologic effects of stress may affect all stages of wound healing in some capacity. In stressed patients, immunologic (T cell phenotypes) / cytokine (low interleukin-1-alpha and platelet-derived growth factor) dysregulation, decreased expression of regenerative factors (basic fibroblast growth factor), tissue hypoxia, dysregulation of cellular mobility and metabolomic kinetics, and matrix metalloprotease activity are detected during the various phases of wound healing [27-29].
Both increase in glucocorticoid and catecholamine production can also delay soft tissue wound-healing responses. Hence, care must be taken when performing periodontal/implant surgery on a patient who is extremely stressed or on someone who is in a high-stress environment. Important factors to take into account include primary wound closure, a longer healing time, antibiotic coverage, limiting extensive and lengthy surgical procedures, or even delaying the surgery to a time when the patient’s life is less stressful.
Stress-biofilm interconnection
With reduced immunity there increases the susceptibility of increase in proliferation of notorious periodontal pathogenic bacteria namely Red complex bacteria [10,30]. These pathogens are found in subgingival plaque of patients with periodontitis and related with the levels of oxidative stress markers like saliva i.e. 8-hydroxydeoxyguanosine and malondialdehyde [31]. Moreover, studies have found correlation of cortisol levels and presence of P. gingivalis found in subgingival plaque of localized periodontitis with respect to age, sex, income and smoking status [10,32]. Moreover another study highlighted the fact that cortisol when administered ex vivo causes change in gene expression of oral microbiome and thus causing dysbiosis in oral milieu that paves way for the progression of periodontal disease [33]. P. gingivalis one of the red complex microorganisms is known to induce inflammation by modulating. Toll like receptors via virulence factors called gingipains which converts complement C5 to C5a [4,10]. Currently, it is also found that stress and inadequate coping or social support can cause activation of herpes virus [4]. While in aggressive periodontitis, there is higher load of Epstein-Barr virus and cytomegalovirus but latent herpes virus infection are more common in chronic periodontitis and gingivitis [34].
Stress and gingival circulation
It has been found that the tonicity of blood vessel is controlled via autonomic nervous system which gets activated in response to stress [15]. Thus, prolonged stress can cause constriction of blood vessels that supplies gingival tissue and thereby hampers oxygen and nutrient supply to gingiva.
Stress and soft tissue wound healing
As immune response plays a pivotal role in wound healing and thereby becomes a bonafide factor for determining prognosis of periodontal therapy. Cytokines such as IL-1, IL-8 and TNF-alpha are responsible for clearing of damaged tissue and promote new tissue formation by recruiting fibroblast and epithelial cells are reduced in response to stress [27]. Moreover stress also suppresses mitogen stimulation, antibody and cytokine production and NK cell activity [27]. Catechcolamine on the other hand also causes peripheral vasoconstriction which further hampers the oxygen dependent healing mechanisms.
Stress and hard tissue wound healing
Bone tissue homeostasis is a balance between resorption and formation that is mediated by coupling mechanism. Healing of alveolar bone after periodontal damage or surgery, including implant placement, necessitates a shift in the osteoid cycle balance towards greater bone reconstructive activity (i,e., high osteoprotegerin) and decreased bone resorptive activity (i,e., low RANKL expression). Interestingly, chronic stress can disrupt this crucial osteoid cycle, impacting osteoid competence by changing the ratio of formative or resorptive lineage cells in the bone. Moreover, chronic stress disorders are also associated with poor alveolar bone growth and osteoporosis [35].
Health-impairing behaviors in stress
In addition to its biochemical effects, chronic stress may promote the adoption of damaging behaviors, such as increased smoking or alcohol consumption, inadequate sleep, poor dietary choices, deficient hygiene practices, or reluctant to follow postoperative instructions and recall visits. All of these factors are strong predictors of microbial dysbiosis and have been linked to negative health outcomes such as obesity, high blood pressure, severe periodontal disease, and tooth loss [36,37].
Classification of stress for treating periodontal/implant patient
Chronic stress affects each individual differently because the body has an inbuilt buffering reserve capacity to maintain a balance of the circulating hormones/chemokines. A classification of stress-related disorders based on neurologic activity as measured by an electroencephalogram and learning algorithms may be required to distinguish the biologic impacts of stress on systemic as well as periodontal health [38]. Tier 1 patients with low levels of chronic stress (eg, loss of relative, or financial crisis) who have developed coping mechanisms to minimize the biologic/systemic effects require regular monitoring of their coping strategies and resources for living. In patients with high levels of chronic stress (Tier 2), who have not established coping mechanisms, definitive stress management therapy is required for coping with stressors; this includes regular exercise, adequate sleep, quality nutrition, daily meditation, and avoiding enabling substances such as caffeine and alcohol.
Treatment strategies for chronic stress in periodontal patients
Prevention measures are the most effective to treat periodontal diseases in all individuals who suffer from chronic stress. Short periodontal maintenance recalls, motivation for proper oral hygiene, patient well-being, and reduced pain experience are critical components in the treatment protocol. Chronic stress can have a negative impact on a person’s ability to make decisions. If a scenario arises, these individuals should be referred for counseling or medical services (such as smoking cessation, sleep therapy, etc.) for a better periodontal treatment outcome. Moreover, Yoga/meditation for treating periodontal disease in chronic stress patients demonstrated enhanced treatment outcomes by battling stress concurrently with periodontal treatments [39]. When a patient with chronic stress seeks periodontal therapy, it is critical to diagnose and address the underlying cause using conservative treatment procedures. Some additional considerations include scheduling appointments early in the morning to avoid waiting anxiety, prophylactic antibiotics, antimicrobial oral rinses, and low-dose doxycycline to suppress inflammatory mediators during the initial stages of healing.
Conclusion
Chronic stress, like other modifiable factors (such as smoking), has been shown to have an important role in the progression of chronic periodontitis. However, due to a lack of reliable assessment criteria, quantifying stress in daily practice has become extremely difficult. However, it has been demonstrated that chronic stress has a significant negative impact on periodontal health via a complex neuro-endocrine pathway that alters biofilm formation, causing dysbiosis of the microbial niches and ultimately leading to periodontal disease progression. Furthermore, it has been shown to alter gingival circulation and impair normal wound healing, complicating the prognosis of periodontal treatment. De-escalation of chronic stress situations is an effective therapy for chronic stress patients. Therefore, as healthcare providers, we must take steps to include knowledge regarding the accurate assessment of stress levels so that we may alter our therapeutic strategies to ensure that periodontal diseases can be effectively treated.
References
- Decker A, et al. The assessment of stress, depression, and inflammation as a collective risk factor for periodontal diseases: a systematic review. J Clin Oral Investig. 2020; 24(1): 1-12.
- Gomaa N, et al. Stressed-out Oral immunity: A gateway from socioeconomic adversity to periodontal disease. Psychosom Med. 2020; 82(2): 126-137.
- Goetzal RZ, Pei X, Tabrizi MJ, et al. Ten modifiable risk factor are linked to more than one-fifth of employer-employee health care spending. Health Aff (Millwood). 2012; 31: 2474-2484.
- Warren KR, Postolache TT, Groer ME, et al. Role of chronic stress and depression in periodontal diseases. Periodontol 2000. 2014; 64:127-38. doi: 10.1111/prd.12036.
- Lazarus RS, Folkman S. Stress, appraisal and coping. New York: Springer. 1984.
- Sachin Goyal, Garima Gupta, Betsy Thomas, et al. Stress and periodontal disease: The link and logic!! Ind Psychiatry J. 2013; 22(1): 4-11.
- Selye H. The Stress of Life. NY, Mc Graw Hills Editors, c system. 1956.
- World health organization definition of stress. Accessed via: https://www.who.int/news-room/questions-and-answers/item/stress.
- Du Mont KA, Widom CS, Czaja SJ. Predictors of resilience in abused and neglected children grown up: the role of individual and neighborhood characteristics. Child abuse Negl. 2007; 31: 255-74.
- Anna M Spector, Teodor T Postolache, Faisal Akram, et al. Psychological stress: A predisposing and exacerbating factor in periodontitis. Current Oral Health Reports. 2020; 7: 208-215.
- Cohen S, Tyrrell DA, Smith AP. Psychological stress and susceptibility to the common cold. N Engl J Med. 1991: 325: 606-612.
- Mithlesh Bhagat, Roopali Tapashetti, Ghousia Fatima. Effect of stress over Periodontium. Gal Int J Health Sci Res. 2020; 5: 46-57.
- Deinzer R, Kleinedsm C, Stiller-Winkler R, et al. Prolonged reduction of salivary immunoglobulin-A after a major academic test. Intj Psychopysiol. 2000; 37: 219-232.
- Page RC, Engel LD, Narayana AS, et al. Chronic inflammatory gingival and periodontal disease. Jama. 1978; 11:545-50.
- Gerard J Linden, Brian H Mullally, Ruth Freeman. Stress and the progression of periodontal disease. J Clin Periodontol. 1996; 23(7): 675-80.
- Cohen S, Gianaros P, Manuck S. A stage model of stress and disease. Perspectives on Psychological Science. 2016; 11: 456-463.
- Alexandra D Crosswell, Kimberly G Lockwood. Best practices for stress measurement: How to measure psychological stress in health research Health Psychol open. 220; 7(2): 2055102920933072
- Vasiliou, K Shankardass, R Nisenbaum. Current stress and poor oral health. BMC Oral Health. 2016; 16: 88.
- Acute and chronic stress definition accessed via:https://www.psychology.org.au/for-the-public/Psychology-topics/Stress/Types-of-stress.
- Segerstrom SC, Miller GE. Psychological stress and the human immune system: a meta-analytic study of 30 years of inquiry. Psychol Bull. 2004; 130(4): 601.
- Frédéric Dutheil, Sarah de Saint Vincent, Bruno Pereira, et al. DHEA as a Biomarker of Stress: A Systematic Review and Meta-Analysis. Front Psychiatry. 2021; 12: 688367.
- Steptoe A, Hamer M, Chida Y. The effects of acute psychological stress on circulating inflammatory factors in humans: A review and meta-analysis. Brain Behav Immun. 2007; 21(7): 901-12.
- Page RC. The role of inflammatory mediators in the pathogenesis of periodontal disease. J periodontal Res. 1991; 26(3): 230-42.
- Felten D, et al. Noradrenergic and peptidergic innervation of lymphoid tissue. J Immunol. 1985; 135(2 Suppl): 755s-765s.
- Arnone D, et al. State-dependent changes in hippocampal grey matter in depression. Mol Psychiatry. 2013; 18(12): 1265-1272.
- Wang, H.L., Decker, A.M. Effects of Occlusion on Periodontal Wound Healing. Compend Contin Educ Dent. 2018; 39(9): 608-612.
- Glaser R, et al. Stress-related changes in proinflammatory cytokine production in wounds. Arch Gen Psychiatry. 1999; 56(5): 450-456.
- Zhao Y-J, et al. Psychological stress delays periodontitis healing in rats: the involvement of basic fibroblast growth factor. Mediators Inflamm. 2012; 2012.
- Gajendrareddy PK, et al. Hyperbaric oxygen therapy ameliorates stress-impaired dermal wound healing. Brain Behavior Immunity. 2005; 19(3): 217-222.
- Socransky SS, Haffajee AD, Cugini MA, et al. Microbial complexes in subgingival plaque. J Clin Periodontal.1998; 25(2): 134-44.
- Almerich-Silla JM, Montiel - Company JM, Pastor S, et al. Oxidative stress parameters in saliva and its association with periodontal disease and types of bacteria. Dis Markers. 2015; 2015: 653537.
- Adrila CM, Guzman IC. Association of Porphyromonas gingivalis with high levels of stress induced hormone cortisol in chronic periodontitis patients. Investig Clin Dent. 2016; 7(4): 361-7.
- Duran-Pinedo AE, Solbiati J, Frias-Lopez J. The effect of the stress hormone cortisol on the metatranscriptome of the oral microbiome. Npj Biofilms and mIcrobiomes. 2018; 4(1): 25.
- Slots J. Herpesviral-bacterial interactions in periodontal diseases. Periodontal. 2010; 52: 117-140.
- Glaesmer H, et al. The association of traumatic experiences and posttraumatic stress disorder with physical morbidity in old age: A German population-based study. Psychosom Med. 2011; 73(5): 401-406
- Costa FO, et al. Effect of compliance during periodontal maintenance therapy on levels of bacteria associated with periodontitis: A 6-year prospective study. J Periodontol. 2018; 89(5): 519-530.
- Copeland LB, et al. Predictors of tooth loss in two US adult populations.J Public Health Dent. 2004; 64(1): 31-37.
- Friedman A, et al. Chronic stress alters striosome-circuit dynamics, leading to aberrant decision-making. Cell. 2017; 171(5): 1191-1205.e28.
- Sudhanshu A, et al. Impact of yoga on periodontal disease and stress management. Int J Yoga. 2017; 10(3): 121.