
SciBase Journals
SciBase Clinical and Medical Case Reports
ISSN 2995-5874
- Article Type: Case Report
- Volume 2, Issue 4 - 2024
- Received: Jul 11, 2024
- Accepted: Sep 16, 2024
- Published Online: Sep 23, 2024
Character Meets Anatomy: Ten Times Typical DCIs; Case Report
Jochen D Schipke*
Research Group Experimental Surgery, University Hospital, Düsseldorf, Germany.
*Corresponding Author: Jochen D Schipke
Research Group Experimental Surgery, University Hospital, Düsseldorf, Germany.
Email: j.schipke@gmx.org
Abstract
An open (Persistent) Foramen Ovale (PFO) is a known risk factor for the development of Decompression Illnes (DCI) in the context of scuba diving. The typical manifestations of PFO-associated DCI encompass cutaneous and vestibular symptoms. Despite this, the efficacy of PFO closure remains a subject of ongoing debate. Furthermore, PFO closure does not guarantee immunity against DCI. Consequently, individuals engaging in diving activities post-PFO closure should exercise caution, refraining from aggressive dives and adhering to the principles of low-bubble diving as outlined by SUHMS guidelines.
In this case report an experienced technical diver with 5,000+ dives suffered several times a typical DCI. In a university clinic setting, a PFO was identified and sub¬sequently occluded. Nevertheless, further DCI occurred after the intervention, although in the control test after PFO closure, no bubbles migrated from right to left. In the first bubble testing there were no findings of pulmonary shunts. It remains unclear if the patient is a high-bubbler or if he has dynamic Intrapulmonal Arteriovenous (IPAV) anastomoses while diving that cannot be detected at rest. Another aspect is his fit for diving certification, which is meanwhile refused by some experts.
Keywords: Scuba diving; Decompression illness; Patent foramen ovale; Intrapulmonal arterio-venous nastomoses; Conservative diving.
Citation: Schipke JD. Character Meets Anatomy: Ten Times Typical DCIs; Case Report. SciBase Clin Med Case Rep. 2024; 2(4): 1031.
Case presentation
During scuba diving, formation of nitrogen bubbles might induce decompression sickness [1,2]. As a reason for the crossover of nitrogen bubbles from the venous to the arterial vascular system there are possible mechanisms such as pulmonary shunting, anatomical shunting through arteriovenous anastomosis and finally the most common reason intracardial shunting. Here a patent (Persistent) Foramen Ovale (PFO) has been described unanimously for decades [3-5].
Such an interatrial shunt exists also in adults. Its incidence greatly varies: from 25% up to 40% [6,7]. The risk for suffering from DCI in divers with PFO might be mitigated by two interventions: PFO closure or conservative diving [8,9]. Unfortunately, PFO closure does not fully protect against DCI [10]. Based on the mismatch between the high prevalence of PFO and low incidence of DCI, it is suggested that primary screening for PFO should not be carried out on a routine basis in divers [11].
Beside PFO, intrapulmonary shunts in SCUBA diving present another risk factor for venous bubbles to become arterialized [12-14].
In the present case, the diver had a typical right to left shunt through a PFO with no additional pulmonary shunts. The PFO was diagnosed using transoesophageal echocardiography. A suture-mediated PFO closure was performed that represents a safe alternative to traditional umbrella-like devices [15,16]. Despite this, subsequent severe Decompression Sickness (DCI) incidents were observed. The following will first describe the entire series of ten diving accidents and attempt to explain how they could have occurred.
Demographics: The diver has a height of 1.89 m and a body mass of 95 kg, resulting in a BMI of 26.3 kg/m². The diver has completed around 5,500 dives within his long diving history. He is a nonsmoker, has a hyperlipemia treated with a statin and no further diseases, no allergies. Since decades, he works as a professional cave instructor.
Already at the age of 18, the diver experienced cutaneous decompression sickness following incorrect instructions on the dive table provided by an instructor (Table 1). Over the years, the diver experienced seven neurological Decompression Incidents (DCI). The second one happening at his age of 26 years after a 32 min cave dive to 50 m, necessitating three sessions in a hyperbaric chamber and additional sessions two days later. Likely, this severe DCI was triggered by a CO-intoxication, as a later breathing gas analysis revealed CO impurity.
Table 1: Years and locations of ten DCIs.
| DCI | Date | Location | Type | Depth [m] | Duration [min] | Breathing gas | Therapy |
|---|---|---|---|---|---|---|---|
| 1 | 1987 | Open water | DCI I | 31 | 32 | Air | none |
| 2 | 1996 | Cave | DCI II | 50 | 32 | Air | HBO |
| 3 | 2006 | Cave | DCI II | 91 | 107 | CCR-Trimix | NBO |
| 4 | 2006 | Open water | DCI II | 74 | 96 | CCR-Trimix | NBO |
| 5 | 2011 | Open water | DCI II | 46 | 37 | Air, NX-50 | NBO |
| 6 | 2015 | Mine, DE | DCIII | 43 | 83 | Air-CCR | NBO |
| 7 | 2015 | Mine, DE | DCI II | 70 | 101 | TMX-CCR | HBO |
| 2018 PFO closure | |||||||
| 8 | 2019 | Mine, DE | DCI | 36 | 34 | |
NBO |
| 9 | 2019 11:00 13:00 14:10 16:00 |
Mine, DE |
DCI DCI |
25 25 25 25 |
41 39 37 43 |
Nitrox* Nitrox* Nitrox* Nitrox* |
NBO |
| 10 | 2019 | Mine, DE | DCI | 25 | 30 | Nitrox* | |
| 11 | 2019 | Lake, DE | ** | 7 | 33 | Air | none |
In case Nitrox was breathed, max. PO2 of 1.3 bar. *DCS-like symptoms after pressurizing the heating accumulator on a nerve.
Anamnesis: In order to identify any underlying causes for the subsequent DCIs, a Transoesophageal Echocardiogram (TEE) was conducted after a PFO had been primarily excluded in a previous medical examination but with limited diagnostic possibilities. This time, a relevant PFO was discovered, which showed spontaneous bubble transfer after bubbling but no pulmonary shunts. Consequently, the PFO was occluded in 2018 via stitching technique.
On one dive after the PFO closure - DCI #8 in 2019 - DCI symptoms recurred. Nevertheless, the diver proceeded to perform additional dives with similar profiles one and four days later.
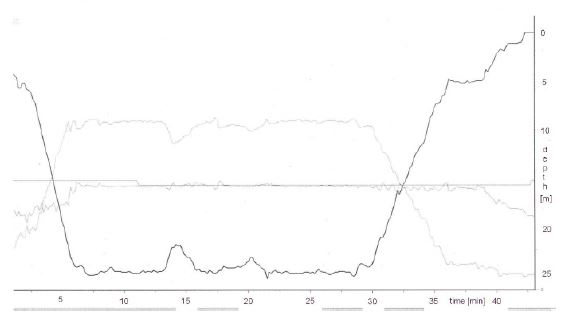
Accident ‘#9’ The diver conducted four dives on the subsequent day using a rebreather, maintaining a maximum PO2 between 1.2 and 1.3 bar. Each dive reached a maximum depth of 25 m with an average dive time of 40 min, all completed within a span of 5:45 h. Despite being no-decompression dives, a safety stop was consistently observed (Figure 1). During the third dive of the day, the diver began experiencing initial symptoms of DCI, feeling a slight tingling sensation below the belly button marking the occurrence as DCI ‘#9’. Despite this, the diver proceeded to undertake another similar dive, being accompanied by two students. Interestingly, the symptoms neither improved nor deteriorated throughout the entire dive.
Approximately 30 min after that dive and a warm shower, additional reddening in that area was observed, while the tingling sensation intensified.
Therapy/examinations: Five days after the accident, the diver underwent seven successful Hyperbaric Oxygen (HBO) sessions. As a result, his symptoms improved to a certain extent, leading to his discharge. Prior to this treatment, no neurological intervention was deemed necessary.
Around four weeks after the accident, the diver sought a fitness-to-dive certificate at a different hospital. There, he continued to experience occasional tingling sensations and verifiable dorsal column complaints, but without pain or motor impairment. Due to the persistent clinical neurologic (spinal) symptoms following the accident, the university expert group recommended discontinuing diving activities, except for very shallow depths (≤5 m). Additionally, neurological monitoring has been advised.
Approximately three weeks later, a Magnetic Resonance Imaging (MRI) scan of the lumbar spine revealed no lesions of the spinal cord.
After the incident, the diver sought consultation with hyperbaric physicians from another hospital. Given that the MRI revealed no residual radiographic damage, these hyperbaric specialists found no contraindications to continued diving. About ten weeks after the accident, a neurology department at another university clinic found no evidence of central nervous damage, and the diver continued diving until the occurrence of the next DCI-like symptoms that were triggered when a component of his diving gear - the heating accumulator - pressurized a nerve.
Discussion
The subsequent discussion addresses four distinct aspects to elucidate the diver’s Decompression Illnesses (DCIs). Subsequently, two open-ended questions are posed.
High-bubbling: The diver could be a potential high-grade bubbler [17,18], i.e. being more prone to DCI than others. This might not be the case with the diver, as in 2000, he performed several dives in the Lake Constance and consequent Doppler examinations showed no more bubbles than his buddies. Still, this aspect is briefly discussed. A key process is the formation of inert gas bubbles [19]. Bubble formation and DCI occurrence could be linked not “only” to the duration and depth of the dives but also to certain pre-dive conditions [20] and possibly to a specific individual predisposition. It is remembered that DCI is linked not only to bubbles, but also to microparticle release and impaired endothelial function [21].
Exposure to hyperoxia resulting from the on-the-fly nitrox is likely to elevate oxidative stress levels. Especially, when using a rebreather with relatively high PO2 values. In the present case, PO2 levels varied only between 1.0 and 1.3 bar. Yet, high levels may lead to the production of Reactive Oxygen Species (ROS) that interact with cell structures [22,23]. Vascular gas-bubble formation and hyperoxia may lead to dysfunction of the endothelium. Thus, the antioxidant status of the diver is an important mechanism in the protection against injury.
Incomplete PFO closure: While it may be tempting to consider an recognised PFO closure as flawless, it is crucial to acknowledge that these closures, whether utilizing a suture-mediated PFO closure [24] or an Amplatzer PFO occluder [25], can be incomplete. Contrary to the assumption of complete protection against decompression illness, a study by [10] revealed that four out of 59 patients experienced recurrent DCI despite undergoing PFO closure. To prevent recurrent Decompression illness (DCI) when there might be a residual shunt after PFO closure, a conservative diving profile is suggested.
In postoperative care, it is strongly recommended to conduct a bubble test three months following the procedure to ensure the effectiveness of the PFO closure. Divers are advised against resuming their exercise routine until satisfactory closure is confirmed, as highlighted by [11]. However, it is crucial to note that relying solely on a single post-PFO-closure test, performed shortly after the procedure, may pose risks. Under certain favourable conditions, such as the presence of a substantial volume of Venous Gas Emboli (VGE), arterialization could occur, as pointed out by [26]. Therefore, comprehensive and timely testing protocols are essential to accurately assess the closure status and mitigate potential complications.
It is remembered, that the relation between PFO and DCI incidences is still a matter of discussion. A meta-analysis failed to prove a significant association between PFO existence and DCI [27]. In contrast, a small case-control study demonstrated that clinical manifestations of DCI were significantly more frequent in patients with PFO, compared with those without [26].
In line, a recent European position paper estimated an odds ratio of 5.63 for right to left shunts in patients with DCI, compared with the subjects without [28].
Extracardiac shunts: Intrapulmonary Arterio-Venous Anastomoses (IPAVA) represent another common pathway for a bubble crossover to occur [23,29]. Such IPAVA may - in addition to PFOs - provide a means for VGE to cross over to the arterial circulation due to their larger diameter (>25 μm) compared to pulmonary microcirculation (< 10 μm). When VGE crossover takes place in arterial circulation, bubbles have the potential to cause severe harm as they can be redistributed to the brain, spinal cord and other critical tissues [13]. Of note, in contrast to resting conditions, >95% of healthy humans demonstrate IPAVAs during exercise [30]. i.e. it also applies to demanding SCUBA diving. Rarely there are found other AV shunts in liver or lungs. In this diver they have been excluded by high resolution imaging.
Vulnerable tissue: Maybe the vulnerable tissue is in a damaged precondition and therefore tends to a higher bubbling, on-gassing and off-gassing due to changed perfusion and compartment kinetics. This would possibly lead to an oversaturation [12]. In accident #9, after three/four subsequent dives within 5:45 h, inert gas bubbles will very likely have been released.
Two open-ended questions
How did the diver manage to accumulate about 5.500 dives with only ten instances of DCI despite having a significant and evidently relevant PFO? Furthermore, why did the diver remain unaffected by DCI during considerably deeper, longer, and more strenuous dives beyond 100 m, lasting up to 4 h, and involving multilevel descents? To remember, the presence of a PFO is related to a low absolute risk of suffering five major DCI events per 10,000 dives, the odds of which is five times as high as in divers without PFO [4]. However, until the PFO closure, our diver had already suffered from seven DCIs (Table 1).
DCI #9 occurred after the completion of the third of four training dives within a 5:45 h span, each separated by roughly 20 min of surface interval. Since these dives involved training with students and took place in 8°C water, both the physical exertion and the low water temperature likely contributed to the arterialization of bubbles. The reasons behind the development of DCI for the other dives remain speculative, in particular, considering that this diving procedure had been performed before.
Should the diver be deemed ‘fit-for-dive’? As mentioned before, two divergent opinions emerge from experts affiliated with the hyperbaric facilities of two distinct universities. One perspective asserts that subjecting the spinal cord to a second impact would be intolerable. Consequently, the endorsement of aggressive diving, repetitive or multilevel diving reminiscent of past practices, is strongly discouraged. This caution extends to flat recreational dives of maximum 5 m, as deeper ones pose a potential risk of neurological impacts. The significance of this stance is heightened by the diver’s prospective engagement in teaching cave diving and employing Closed-Circuit Rebreather (CCR) equipment.
Conversely, an opposing viewpoint contends that both the MRI results, which revealed no residual radiographic damage, and an evaluation by another university neurology department, which found no evidence of central nervous system damage, support a different perspective. In light of these findings, these latter experts opted to issue a dive certificate with no imposed restrictions.
Appendix: Following his decompression incident #10 in 2019, the diver has continued diving, even engaging in extended dives, without any further complaints. This positive outcome is due to meticulously adjusting his decompression routines based on a self-authored, highly conservative decompression program including a limitation to maximum two dives per day.
This development is highly gratifying for three reasons: The diver apparently no longer poses a risk to himself. The danger of an own accident leading to a risk for his diving students, is greatly reduced. Ultimately, the medical care - including emergency medicine - with its high costs that would have to be borne by the public, is no longer necessary.
Conclusions
The occurrence of the first seven cases of Decompression Illness (DCI) in this diver can be reasonably attributed to two primary factors. The first factor is their predisposition to bubble formation, commonly referred to as ‘bubbling’. The second factor is the presence of an arterio-venous shunt through a Persistent Foramen Ovale (PFO).
The closure of the PFO has proven to be a sensible intervention, as it reduces the risk of DCI to a level comparable to that of other divers who do not have a right-to-left shunt. However, it is important to note that closure of the shunt does not completely eliminate the risk of a diver experiencing DCI through other mechanism.
As a result, the adoption of conservative diving practices serves as another senseful intervention, although low bubble diving recommendations do not exist for technical diving. Conservative recreational diving significantly reduces the risk of recurrent DCI. It remains unclear how to deal with a fit for dive certification in such complex divers.
A cardiologist friend always says: “Closing a PFO doesn’t protect against DCI. It’s the bubbles that need to be minimized!”
References
- Nakayama H, Shibayama M, Yamami N, Togawa S, Takahashi M, et al. Decompression sickness and recreational scuba divers. Emergency Medicine Journal : EMJ. 2003; 20(4): 332-334. https://doi.org/10.1136/emj.20.4.332.
- Brebeck AK, Deussen A, Range U, Balestra C, Cleveland S, et al. Beneficial effect of enriched air nitrox on bubble formation during scuba diving. An open-water study. Journal of Sports Sciences. 2018; 36(6): 605-612. https://doi.org/10.1080/02640414.2017.1326617.
- Bove AA. Risk of decompression sickness with patent foramen ovale. Undersea & Hyperbaric Medicine: Journal of the Undersea and Hyperbaric Medical Society, Inc. 1998; 25(3): 175-178.
- Torti SR, Billinger M, Schwerzmann M, Vogel R, Zbinden R, et al. Risk of decompression illness among 230 divers in relation to the presence and size of patent foramen ovale. European Heart Journal. 2004; 25(12): 1014-1020. https://doi.org/10.1016/j.ehj.2004.04.028.
- Liou K, Wolfers D, Turner R, Bennett M, Allan R, et al. Patent foramen ovale influences the presentation of decompression illness in SCUBA divers. Heart, Lung & Circulation. 2015; 24(1): 26-31. https://doi.org/10.1016/j.hlc.2014.07.057.
- Torbey E, Thompson PD. Patent foramen ovale: Thromboembolic structure or incidental finding? Connecticut Medicine. 2011; 75(2): 97-105.
- Sramek M, Honek J, Tomek A, Ruzickova T, Honek T, et al. Risk stratification of neurological decompression sickness in divers. Bratislava Medical Journal. 2022; 123(02): 77-82. https://doi.org/10.4149/BLL_2022_022.
- Anderson G, Ebersole D, Covington D, Denoble PJ. The effectiveness of risk mitigation interventions in divers with persistent (patent) foramen ovale. Diving and Hyperbaric Medicine. 2019; 49(2): 80-87. https://doi.org/10.28920/dhm49.2.80-87.
- Wilmshurst P. Risk mitigation in divers with persistent (patent) foramen ovale. Diving and Hyperbaric Medicine. 2019; 49(2): 77-78. https://doi.org/10.28920/dhm49.2.77-78.
- Vanden Eede M, Van Berendoncks A, De Wolfe D, De Maeyer C, Vanden Eede H, et al. Percutaneous closure of patent foramen ovale for the secondary prevention of decompression illness in sports divers: Mind the gap. Undersea & Hyperbaric Medicine: Journal of the Undersea and Hyperbaric Medical Society, Inc. 2019; 46(5): 625-632.
- Smart D, Mitchell S, Wilmshurst P, Turner M, Banham N. Joint position statement on Persistent Foramen Ovale (PFO) and diving. South Pacifi c Underwater Medicine Society (SPUMS) and the United Kingdom Sports Diving Medical Committee (UKSDMC). Diving and Hyperbaric Medicine. 2015; 45(2): 129-131.
- Hartig F, Reider N, Sojer M, Hammer A, Ploner T, et al. Livedo Racemosa-The Pathophysiology of Decompression-Associated Cutis Marmorata and Right/Left Shunt. Frontiers in Physiology. 2020; 11: 994. https://doi.org/10.3389/fphys.2020.00994.
- Madden D, Ljubkovic M, Dujic Z. Intrapulmonary Shunt and SCUBA Diving: Another Risk Factor? Echocardiography. 2015; 32(S3). https://doi.org/10.1111/echo.12815.
- Wilmshurst PT, Morrison WL, Walsh KP. Comparison of the size of persistent foramen ovale and atrial septal defects in divers with shunt-related decompression illness and in the general population. Diving and Hyperbaric Medicine. 2015; 45(2): 89-93.
- Cannata F, Stankowski K, Donia D, Figliozzi S, Fazzari F, et al. Percutaneous suture-based patent foramen ovale closure: A state-of-the-art review. Trends in Cardiovascular Medicine. 2023; S1050173823000956. https://doi.org/10.1016/j.tcm.2023.10.004.
- Neto A, Resende CX, Tavares Silva M, Silva JC, Macedo F. A new era in patent foramen ovale closure - a percutaneous suture-based ‘deviceless’ technique (NobleStitch®): Experience of a Portuguese center. Revista Portuguesa de Cardiologia. 2023; 42(1): 53-59. https://doi.org/10.1016/j.repc.2021.08.015.
- Cialoni D, Pieri M, Balestra C, Marroni A. Flying after diving: Should recommendations be reviewed? In-flight echocardiographic study in bubble-prone and bubble-resistant divers. Diving and Hyperbaric Medicine. 2015; 45(1): 10-15.
- Arieli R, Khatib S, Vaya J. Ovine plasma dipalmitoylphosphatidylcholine does not predict decompression bubbling. Respiratory Physiology & Neurobiology. 2019; 259: 26-29. https://doi.org/10.1016/j.resp.2018.06.013.
- Møllerløkken A, Gaustad SE, Havnes MB, Gutvik CR, Hjelde A, et al. Venous gas embolism as a predictive tool for improving CNS decompression safety. European Journal of Applied Physiology. 2012; 112(2): 401-409. https://doi.org/10.1007/s00421-011-1998-9.
- Theunissen S, Balestra C, Boutros A, De Bels D, Guerrero F, et al. The effect of pre-dive ingestion of dark chocolate on endothelial function after a scuba dive. Diving and Hyperbaric Medicine. 2015; 45(1): 4-9.
- Barak OF, Janjic N, Drvis I, Mijacika T, Mudnic I, et al. Vascular dysfunction following breath-hold diving. Canadian Journal of Physiology and Pharmacology. 2020; 98(2): 124-130. https://doi.org/10.1139/cjpp-2019-0341.
- Madden LA, Laden G. Gas bubbles may not be the underlying cause of decompression illness - The at-depth endothelial dysfunction hypothesis. Medical Hypotheses. 2009; 72(4): 389-392. https://doi.org/10.1016/j.mehy.2008.11.022.
- Brubakk AO, Ross JAS, Thom SR. Saturation diving; physiology and pathophysiology. Comprehensive Physiology. 2014; 4(3): 1229-1272. https://doi.org/10.1002/cphy.c130048.
- Ruiz CE, Kipshidze N, Chiam PTL, Gogorishvili I. Feasibility of patent foramen ovale closure with no‐device left behind: First‐ in‐man percutaneous suture closure. Catheterization and Cardiovascular Interventions. 2008; 71(7): 921-926. https://doi.org/10.1002/ccd.21550.
- Madhkour R, Wahl A, Praz F, Meier B. Amplatzer patent foramen ovale occluder: Safety and efficacy. Expert Review of Medical Devices. 2019; 16(3): 173-182. https://doi.org/10.1080/17434440.2019.1581060.
- Germonpre P. Persistent (patent) foramen ovale (PFO): Implications for safe diving. Diving and Hyperbaric Medicine. 2015; 45(2): 73-74.
- Lairez O, Cournot M, Minville V, Roncalli J, Austruy J, et al. Risk of Neurological Decompression Sickness in the Diver with a Right-to-Left Shunt: Literature Review and Meta-Analysis. Clinical Journal of Sport Medicine. 2009; 19(3): 231-235. https://doi.org/10.1097/JSM.0b013e31819b0fa2.
- Pristipino C, Germonpré P, Toni D, Sievert H, Meier B, et al. European position paper on the management of patients with patent foramen ovale. Part II - Decompression sickness, migraine, arterial deoxygenation syndromes and select high-risk clinical conditions. European Heart Journal. 2021; 42(16): 1545-1553. https://doi.org/10.1093/eurheartj/ehaa1070.
- Schipke JD, Tetzlaff K. Why predominantly neurological decompression sickness in breath-hold divers? Journal of Applied Physiology (Bethesda, Md. 1985). 2016; 120(12): 1474-1477. https://doi.org/10.1152/japplphysiol.00840.2015.
- Lovering AT, Duke JW, Elliott JE. Intrapulmonary arteriovenous anastomoses in humans - response to exercise and the environment. The Journal of Physiology. 2015; 593(3): 507-520. https://doi.org/10.1113/jphysiol.2014.275495.