
SciBase Journals
SciBase Clinical and Medical Case Reports
ISSN 2995-5874
- Article Type: Case Report
- Volume 2, Issue 4
- Received: Oct 06, 2024
- Accepted: Nov 19, 2024
- Published Online: Nov 26, 2024
Situs Inversus Totalis with Inguinal Hernia: A Case Report
Yingsen Pan1; Yi Shen1; Feipeng Qin1; Xiaoming Ying2*
1The 3rd Clinical Medical College, Zhejiang Chinese Medical University, Hangzhou, China.
2The 3rd Affiliated Hospital, Zhejiang Chinese Medical University, Hangzhou, China.
*Corresponding Author: Xiaoming Ying
The 3rd Affiliated Hospital, Zhejiang Chinese Medical University, Hangzhou, China.
Email: 28588509@qq.com
Abstract
Indirect inguinal hernia is a common surgical condition, and surgery is generally the preferred treatment option. Total situs inversus is extremely rare in clinical practice. Here, we present a case of total situs inversus with an indirect inguinal hernia. Considering the literature analysis of situs inversus, patients with this condition are prone to complications during surgery due to the abnormal anatomical position, posing significant challenges for surgeons. When treating such patients, it is essential to enhance relevant auxiliary examinations and thoroughly consider all potential scenarios.
Keywords: Situs inversus; Inguinal hernia; Dextrocardia; Imaging; Case report.
Citation: Pan Y, Shen Y, Qin F, Ying X. Situs Inversus Totalis with Inguinal Hernia: A Case Report. SciBase Clin Med Case Rep. 2024; 2(4): 1033.
Case presentation
A 66 years old male patient, who complained of a reproducible mass in the right inguinal region for more than 30 years, was hospitalied in the 3rd affiliated hospital of Zhejiang Chinese Medical University.
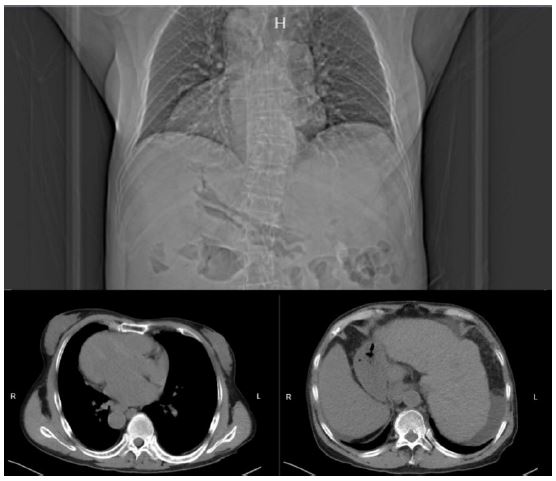
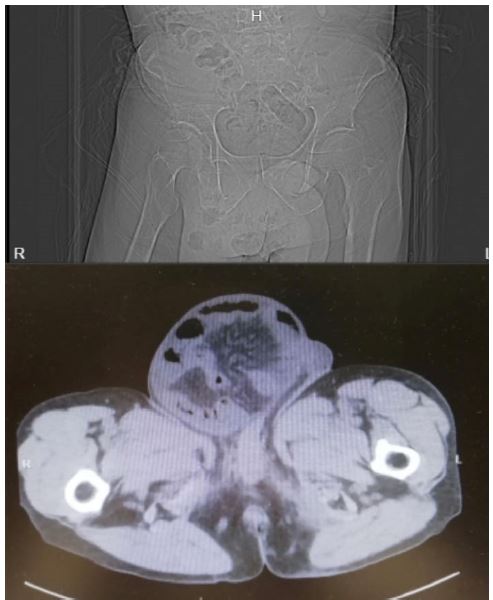
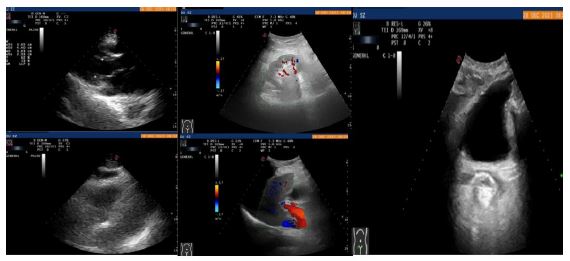
Physical examination: A 14 cm x 15 cm ovoid mass was discovered in the right inguinal region. It exhibited a soft texture, smooth surface, no tenderness, and a clear boundary. The mass reduced when the patient lay flat and could be retrograded into the abdominal cavity through the subcutaneous ring. The exploration revealed a wide and loose subcutaneous ring, confirmed by a positive translucency test. No palpable abnormalities were found in the left inguinal region. The abdomen was soft and non-tender, with normal bowel sounds of about 3 to 4 beats per minute. The patients were admitted to the hospital to complete the relevant auxiliary examinations. The electrocardiogram showed dextrocardia. A few fibrous lesions in both lungs, situs inversus, enlarged heart, liver cirrhosis, and splenomegaly were seen on the chest CT (Figure 1). Pelvic CT showed a right inguinal hernia (Figure 2). Ultrasound showed mirrored dextrocardia, hardening of the aorta, Aortic and mitral valve degeneration with mild regurgitation; inversion of liver and spleen, liver cirrhosis, gallbladder wall edema, splenomegaly and widened splenic vein, ascites and crystals in both kidneys (Figure 3). The diagnosis was indirect inguinal hernia, alcoholic cirrhosis with esophageal varices, hepatic encephalopathy, hypersplenism, pulmonary shadow, chronic renal insufficiency, and situs inversus.
Surgical methods: Tension-free repair of right indirect inguinal hernia was performed under general anesthesia. Procedure: After successful anesthesia, the patient was placed in the supine position and made a 2-finger incision from the right pubic tubercle to the midpoint of the right inguinal ligament with a length of 6 cm. The skin, subcutaneous tissue, and aponeurosis of the external oblique muscle of the abdomen were cut, and the spermatic cord was free. The hernia sac was carefully dissociated from the spermatic cord. The hernia sac was ligated at a high level, the sac was inserted back, the mesh was filled, and the transversalis fascia was sutured and fixed. The patch was placed posterior to the spermatic cord, and then sutured and fixed on the pubic tubercle, inguinal ligament and conjoint tendon in turn. The spermatic cord was reduced, the wound and incision were stopped for bleeding, and the tendon and skin of the external oblique muscle were sutured. The operation was successful and the postoperative return was safe.
Discussion
There is no definitive explanation for the etiology of situs inversus, and the known pathogenesis primarily involves gene mutations [1], asymmetric gene expression [2], dysfunctional motor cilia [3], and malrotation of the embryo during development [4]. In general, patients with situs inversus do not show changes in the structure, and without special symptoms [1]. It is usually discovered incidentally when other diseases are accompanied by tests. Partial situs inversus is often associated with severe congenital defects, such as cardiovascular malformations, splenic abnormalities, intestinal torsion and abnormal lung structure [5]. At present, the reports of situs inversus are mostly related to hepatobiliary diseases and heart [6-8]. The examination methods were electrocardiogram, DR, CT and ultrasound.
Situs inversus total viscera with the indirect inguinal hernia was reported for the first time in clinical practice, the association between indirect inguinal hernia and situs inversus lacks sufficient explanation in the current study, which may be attributed to factors such as genetics and gene expression regulation. It provided an opportunity for the medical community to explore. Although in terms of surgery, this patient did not present additional risks and difficulties compared to the non-mirror person. However, if serious complications occur during the operation, such as cardiac arrest, the doctor must understand the mirror state of the patient in advance, so that the correct rescue can be carried out. Due to the anatomical abnormalities, the postoperative recurrence rate of situs inversus with indirect inguinal hernia may be high. Surgeons need to be aware of the possibility of postoperative recurrence and closely monitor the patient’s condition changes during postoperative follow-up.
Declarations
Consent: This is a case report and does not require ethics committee approval. We have de-identified this patient’s details.
Statement and compenting interests: The authors declare that they have no competing interests. Data availability statement the records and data related to this case were kept in the patient records of the Third Affiliated Hospital of Zhejiang Chinese Medical University.
Author contribution conceptualization: Xiaoming Ying, Formal analysis and investigation: Feipeng Qin, Writing- original draft preparation: Yingsen Pan, Writing-review and editing: Yi Shen; Funding acquisition: Xiaoming Ying; Supervision: Xiaoming Ying. All authors have read and approved the final manuscript. Acknowledgements
Funding: This work was supported by Project of famous young and middle-aged TCM doctors in Zhejiang province in 2021(sjzqn202106).
References
- Bisgrove BW, Morelli SH, Yost HJ. Genetics of human laterality disorders: insights from vertebrate model systems. Annu Rev Genomics Hum Genet. 2003; 4: 1-32. doi:10.1146/annurev.genom.4.070802.110428.
- Sutherland MJ, Ware SM. Disorders of left-right asymmetry: heterotaxy and situs inversus. Am J Med Genet C Semin Med Genet. 2009; 151C(4): 307-317. doi:10.1002/ajmg.c.30228.
- Shapiro AJ, Davis SD, Ferkol T, et al. Laterality defects other than situs inversus totalis in primary ciliary dyskinesia: insights into situs ambiguus and heterotaxy. Chest. 2014; 146(5): 1176-1186. doi:10.1378/chest.13-1704.
- Li QS, Liu XG. Situs inversus with hepatobiliary and renal stones: a case report J. Clinical Misdiagnosis and Mistreatment. 2004; (12): 871.
- Kosaki K, Casey B. Genetics of human left-right axis malformations. Semin Cell Dev Biol. 1998; 9(1): 89-99. doi:10.1006/scdb.1997.0187.
- Kyuno D, Kimura Y, Imamura M, et al. Pancreaticoduodenectomy for biliary tract carcinoma with situs inversus totalis: Difficulties and technical notes based on two cases. World J Surg Oncol. 2013; 11: 312. doi:10.1186/1477-7819-11-312.
- Benhammane H, Kharmoum S, Terraz S, et al. Common bile duct adenocarcinoma in a patient with situs inversus totalis: Report of a rare case. BMC Res Notes. 2012; 5: 681. doi:10.1186/1756-0500-5-681.
- Francis RJ, Christopher A, Devine WA, Ostrowski L, Lo C. Congenital heart disease and the specification of left-right asymmetry. Am J Physiol Heart Circ Physiol. 2012; 302(10): H2102-H2111. doi:10.1152/ajpheart.01118.2011.