
SciBase Journals
SciBase Clinical and Medical Case Reports
ISSN 2691-7785
- Article Type: Short Report
- Volume 3, Issue 1
- Received: Sep 03, 2025
- Accepted: Nov 10, 2025
- Published Online: Nov 17, 2025
Man stabs himself, creating a hole in the heart
Yibing Wu1; Xuan Zhang2; Xinlong Liu2*
1Department of Ultrasonic Medicine, Shenzhen Guangming District People’s Hospital, Shenzhen, China.
2Department of Emergency, Shenzhen Guangming District People’s Hospital, Shenzhen, China.
*Corresponding Author: Xinlong Liu
Shenzhen Guangming District People’s Hospital,
Guangming District Huaxia Road 39th, China.
Tel: +8618126081647
Email: liuxinlong0723@sina.com
Abstract
We report a rare case of a 59-year-old male with a history of depression stabbed himself from xiphoid to heart. Following initial cardiothoracic surgery for hemothorax and cardiac repair, the patient was discharged and transferred to a psychiatric facility for depression management. Four weeks later, he returned with complaints of chest pain, cough, and expectoration. Subsequent surgical intervention confirmed these fistulas were secondary to the original stab injury. This case highlights the delayed complications of penetrating cardiac trauma and underscores the importance of multidisciplinary management in such complex scenarios.
Keywords: Pathological channels; Echocardiography; Knife stabbing; Cardiothoracic surgery.
Citation: Wu Y, Zhang X, Liu X. Man stabs himself, creating a hole in the heart. SciBase Clin Med Case Rep. 2025; 3(1): 1034.
Case presentation
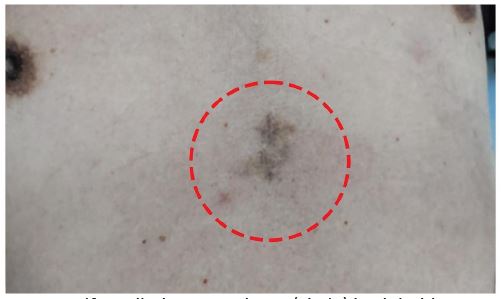
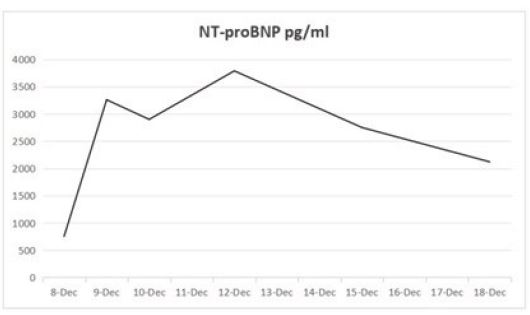
A 59-year-old male with a documented history of depression presented to the emergency department on 7th December with active bleeding and chest pain following a self-inflicted stab wound to the chest (Figure 1). Emergent Video-Assisted Thoracoscopic Surgery (VATS) was performed, including hemothorax evacuation, pericardiotomy with exploration, pulmonary laceration repair, and resection of a premediastinal pericardial hematoma. Postoperatively, the patient was stabilized and transferred to a psychiatric hospital on 19th Dec for specialized care. His laboratory test about N-terminal-pro hormone B-type natriuretic peptide (NT-proBNP) (Figure 2).
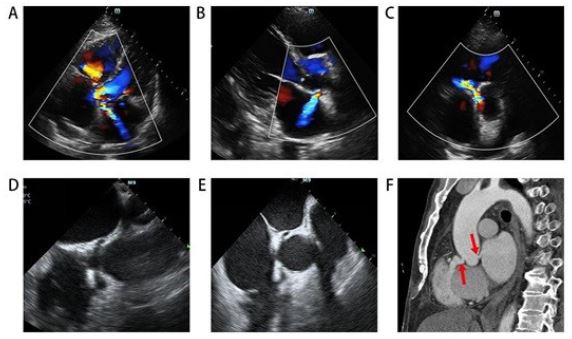
Four weeks later, the patient returned with chest pain, cough, and expectoration. Echocardiography, transesophageal echocardiography, and aortic CTA revealed two abnormal channels from the aortic sinus to the RV and LA (Figure 3). He was transferred to another hospital for cardiothoracic surgery, where surgeons confirmed the channels were caused by the knife stab (Figure 4).
Discussion
Based on the patient’s upper abdominal scar, it is hypothesized that during self-mutilation, the sharp blade penetrated upward from the sub-xiphoid into the cardiac chambers. The trajectory passed through the RV outflow tract into the RV, also perforated the non-coronary sinus of the aorta, and ultimately entered the LA. Given the thin and narrow nature of the blade, the RV wall injury resulted in only minimal pericardial effusion. While the RV wall lesion healed, persistent abnormal intracardiac communications formed two rare pathological channels.
Remarkably, the unique trajectory of the stab wound avoided catastrophic cardiac rupture and strategically bypassed the right coronary artery and critical valvular structures, thereby preventing immediate life-threatening consequences. Now he could care for himself without sequela.

The clinical severity of penetrating cardiac injuries depends on three key factors: anatomical location of injury, defect size, and degree of structural damage to cardiac components [1]. Epidemiological data shows RV injuries are most common (48.6%), followed by Left Ventricle (LV) injuries (47.49%) [2]. Notably, LV ruptures carry higher risks of lethal pericardial hemorrhage and functional impairment compared to RV injuries, with substantially poorer clinical outcomes [3].
Declarations
Conflict of interest: No conflict of interest.
Funding: No funding from an external source supported the publication of this case report.
Ethics approval: We received ethics approval from our institution for reporting this case report.
Consent: Verbal informed consent was obtained from the patient for his anonymized information to be published in this article.
References
- Ferrara M, Baldari B, Vittorio S, Bertozzi G, Cipolloni L, De Simone S. Penetrating cardiac injuries: literature review and analysis of the forensic approach. Front Biosci (Landmark Ed). 2022; 27: 29.
- Isaza-Restrepo A, Donoso-Samper A, Benitez E, Martin-Saavedra JS, Toro A, Ariza-Salamanca DF, et al. Retrospective analysis of 261 autopsies of penetrating cardiac injuries with emphasis on sociodemographic factors. Sci Rep. 2023; 13: 11563.
- Campisi A, Ciarrocchi AP, Grani G, Argnani D, Salvi M, Stella F. Penetrating left ventricular injuries management: single General Thoracic Center experience. Gen Thorac Cardiovasc Surg. 2021; 69: 1254-1257.