
SciBase Journals
SciBase Clinical and Medical Case Reports
ISSN 2691-7785
- Article Type: Case Report
- Volume 3, Issue 1
- Received: Oct 01, 2025
- Accepted: Nov 14, 2025
- Published Online: Nov 21, 2025
A Rare Case of T-Cell Histiocyte Rich Large B-Cell Lymphoma of the Thyroid in a Patient with Hashimoto’s Thyroiditis
Maradana J1; Zainal A2; Kahlon N3*; Velamala P4; Aurora I5; Majety P6; Shaik S7; Torres M7
1Department of Endocrinology, Wentworth Douglass Hospital, Dover NH, USA.
2Department of Endocrinology, Baptist Medical Group, Columbus, MS, USA.
3Department of Medical Oncology, Mass General Cancer Center at Wentworth Douglass Hospital, Dover NH, USA.
4Department of Endocrinology, Central Maine Medical Center, Lewiston, ME, USA.
5Department of Endocrinology, Beverly Hospital, Beverly, MA, USA.
6Division of Endocrinology, Diabetes and Metabolism, Department of Internal Medicine, Virginia Commonwealth University,
Richmond, VA, USA.
7Department of Endocrinology, University of Massachusetts Medical School, Worcester, MA, USA.
*Corresponding Author: Navkirat Kahlon
Department of Medical Oncology, Mass General Cancer Center at Wentworth Douglass Hospital, Dover NH, USA.
Email: navkiratkaurpannu@gmail.com
Citation: Maradana J, Zainal A, Kahlon N, Velamala P, Aurora I, et al. A Rare Case of T-Cell Histiocyte Rich Large B-Cell Lymphoma of the Thyroid in a Patient with Hashimoto’s Thyroiditis. SciBase Clin Med Case Rep. 2025; 3(1): 1035.
Introduction
T-cell/Histiocyte-Rich Large B-Cell Lymphoma (THRLBCL) is a rare and aggressive form of Diffuse Large B-Cell Lymphoma (DLBCL) which usually involves the lymph nodes exclusively with uncommon extranodal involvement. We describe a rare case of a 78-year-old female patient with a history of Hashimoto’s thyroiditis with THRLBCL involving her thyroid gland. To our knowledge, there has only been one other case of a THRBCL arising from the thyroid gland described in the literature [1].
Clinical case
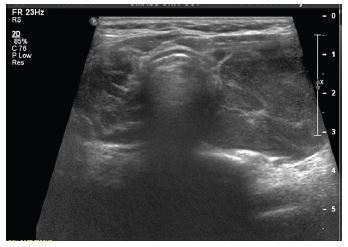
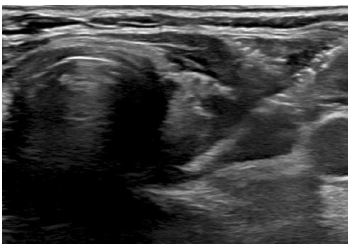
A 78-year-old female with a 10-year history of Hashimoto’s thyroiditis, biochemically on Levothyroxine 75 mcg daily presented to the endocrinology clinic with a 2-month symptom duration of unilateral left sided thyroid fullness and neck discomfort with asymmetric left thyroid enlargement confirmed on physical exam. An Ultrasound (US) of the thyroid and neck was significant for a unilateral increase in the size of the left thyroid lobe from 5.3×3.6×3.3 cm to 8.5×3.3×4.1 cm over 3 years and an enlarged left sided level 3 suspicious cervical lymph node measuring up to 1.4 cm in short axis, with loss of its fatty hilum (Figure 1).
Cytology from a Fine Needle Aspiration (FNA) of the left level 3 cervical lymph node and left thyroid gland showed atypical lymphoid infiltrate featuring scattered large, atypical cells in a background of small lymphocytes. Immunohistochemistry showed labeling for PAX5 and CD20 in the left level 3 cervical lymph node, labeling for PAX5 in the left thyroid FNA and absence of CD30 and CD15. Concurrent flow cytometric studies demonstrated increased CD4 to CD8 ratio amongst the T-cells. Although non-diagnostic, these FNA findings were suspicious for malignancy.
A core needle biopsy of the thyroid and an excisional biopsy of the left level 3 cervical lymph node were performed. Both specimens demonstrated an inflammatory infiltrate of predominantly small lymphocytes and histiocytes, fewer admixed neutrophils, and scattered large highly atypical lymphoid cells. The large, atypical cells showed an intact B-cell program with expression of CD20, CD79a, BOB1, PAX5 and OCT2 and absence of CD30 and CD15 consistent with a diagnosis of THRLBCL (Figure 2).

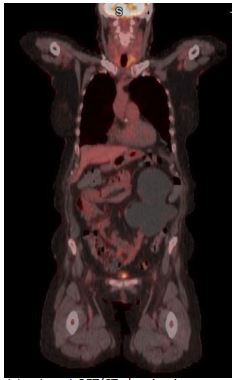
A Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography (FDG PET/CT) scan revealed FDG-avid masses involving the spleen, left thyroid as well as left cervical, supraclavicular, upper mediastinal, and portacaval lymphadenopathy (Figure 3). Her bone marrow biopsy was negative for infiltration of lymphomatous cells.
She was deemed as Stage 3 THRLBCL with International Prognostic Index (IPI) of 2 corresponding with low-intermediate risk cancer. She commenced on 6 cycles of chemotherapy with a combination with Rituximab Cyclophosphamide, Hydroxydaunorubicin Hydrochloride, Vincristine, and Prednisone (R-CHOP).

End of treatment PET scan revealed significant treatment response however there was evidence of residual asymmetric intense FDG uptake in the left thyroid gland (Figure 4). It was uncertain whether the PET findings represented inflammation due to Hashimoto’s thyroiditis versus residual lymphoma. Repeat biopsy of the left lobe showed patchy inflammatory infiltrate that may have been secondary to Hashimoto’s thyroiditis with no clear evidence of lymphoma (Figure 5). Due to the paucity of malignant cells in cases of TCHRBCL, residual lymphoma could not be excluded. Repeat PET scan 12 months later showed increase in size and uptake in her left thyroid gland. A repeat biopsy showed a lymphocytic thyroiditis picture and was negative for malignant cells.
Discussion
THRLBCL is a rare subtype of Diffuse Large B-Cell Lymphoma (DLBCL) involving a limited number of scattered malignant B-cells in a background of T-cells and histiocytes. THRLBCL is often misdiagnosed as Hodgkin’s lymphoma or peripheral T-cell lymphoma due to overlapping pathologic findings [2,3]. The presence of less than 10% (sometime as low as 1%) of large, atypical B-cells in a background rich in T-cells is the unifying feature of the diagnosis [2].
The current case exhibited some unusual pathologic features for TCHRBCL. Usually, background T-cells are predominantly CD8, in contrast to our patient who had predominantly CD4 T-cells [5,6]. Another peculiar feature is that the biopsy specimens demonstrated both scattered small B-cells and large B-cells, a feature that is not typically seen in THRLBCL [6]. A diagnosis of diffuse transformation of nodular lymphocyte predominant Hodgkin lymphoma was considered but the diffuse proliferation outside of follicular dendritic meshworks and involvement of the thyroid gland is not compatible with such diagnosis. Similarly, a diagnosis of follicular helper T-cell lymphoma with admixed large B-cells was considered but while PD1 and CD4 T cells are present, they showed no evidence of immunophenotypic aberrancy by flow cytometry or of clonal T-cell receptor rearrangement by PCR to favor a T-cell lymphoma [5].
The most common primary extranodal sites in THRLBCL included liver, spleen, and bone marrow (each with <10 cases) [4]. THRLBCL involving extranodal sites may thus have uniquely unfavorable biology, potentially explaining poor outcomes reported in prior case series [3,4].
THRLBCL is treated according to stage-matched DLBCL. THRLBCL prognosis has markedly improved with modern rituximab-based immunochemotherapy [4]. Recent advances in immunotherapy have led to significant mortality reductions in melanoma, lung cancer, and lymphomas [7-11]. These improvements underscore the importance of early, accurate diagnosis-particularly in rare presentations-and prompt treatment initiation. However, managing long-term toxicities remains critical as immune-based therapies become increasingly central to cancer care. Unfortunately, CAR-T therapy, which has proven highly effective for patients with relapsed or refractory DLBCL, appears to have limited efficacy in TCHRBCL, hypothesized to be due to the unique tumor microenvironment [12].
Hashimoto’s thyroiditis is considered a risk for thyroid lymphoma usually DLBCL and extra nodal Marginal Zone Lymphoma (MZL) [3]. Its association with TCHRLBL is not well documented [6,11]. The chronic inflammatory stimulus could have contributed to the lymphomagenesis. Notably, lymphoma diagnosis is often unclear on FNA, requiring an excisional biopsy. Malignant lymphomas of the thyroid gland are exceedingly rare, accounting for approximately only 2% of thyroid cancers [1,3]. Of those patients, to our knowledge, the literature describes a single case report of THRLBCL arising from the thyroid gland exclusively [1,3].
Clinicians must maintain an open diagnostic mindset, recognizing that atypical presentations and benign conditions—such as autoimmune thyroiditis—can mimic malignancy both clinically and radiologically. A high index of suspicion, coupled with judicious use of tissue sampling and immunophenotyping, is essential to avoid misdiagnosis and ensure timely, appropriate management [13-16]. This approach underscores the importance of integrating clinical context, imaging findings, and histopathology, particularly when faced with rare entities or discordant features.
Conclusion
In summary, this case highlights an unusual presentation of THRLBCL in the thyroid gland in the setting of Hashimoto’s thyroiditis. The case underscores diagnostic challenges, including limitations of FNA, atypical immunophenotypic features, and difficulties distinguishing residual disease from inflammation on FDG-PET imaging. It also contributes to the limited literature on extranodal THRLBCL involving the thyroid.
References
- Ichikawa S, Watanabe Y, Saito K, Kimura J, Ichinohasama R, Harigae H. T-cell/histiocyte-rich large B-cell lymphoma of the thyroid. Exp Hematol Oncol. 2013; 2: 1.
- Pittaluga S, Jaffe ES. T-cell/histiocyte-rich large B-cell lymphoma. Haematologica. 2010; 95: 352-356.
- Weshi AE, Akhtar S, Mourad WA, Ajarim D, Abdelsalm M, Khafaga Y, et al. T-cell/histiocyte-rich B-cell lymphoma: clinical presentation, management, and prognostic factors: report on 61 patients and review of literature. Leuk Lymphoma. 2007; 48: 1764-1773.
- Ollila TA, Reagan JL, Olszewski AJ. Clinical features and survival of patients with T-cell/histiocyte-rich large B-cell lymphoma: analysis of the National Cancer Data Base. Leuk Lymphoma. 2019; 60: 3426-3433.
- Ohgami RS, Zhao S, Natkunam Y. Large B-cell lymphomas poor in B cells and rich in PD-1+ T cells can mimic T-cell lymphomas. Am J Clin Pathol. 2014; 142: 150-156.
- Kunder C, et al. Predominance of CD4+ T cells in T-cell/histiocyte-rich large B-cell lymphoma and identification of a subset of patients with peripheral B-cell lymphoma. Am J Clin Pathol. 2017; 147: 596-603.
- Kahlon N, Doddi S, Yousif R, Najib S, Sheikh T, Abuhelwa Z, Burmeister C, Hamouda DM. Melanoma treatments and mortality rate trends in the US, 1975 to 2019. JAMA Netw Open. 2022; 5: e2245269.
- Kundu R, Kal N, Singh A, Jagadeesh D. Global incidence, mortality and risk factors of Hodgkin’s and non-Hodgkin’s lymphoma 1990–2021: a global health data study. Blood. 2024; 144: 6360.
- Howlader N, Forjaz G, Mooradian MJ, Meza R, Kong CY, Cronin KA, Mariotto AB, Lowy DR, Feuer EJ. The effect of advances in lung-cancer treatment on population mortality. N Engl J Med. 2020; 383: 640-649.
- Qureshi Z, Jamil A, Hameed F, Kahlon N. Advancements in cutaneous T-cell lymphoma treatment: unveiling novel therapeutic avenues and clinical implications. Am J Clin Oncol. 2025.
- Abuhelwa Z, Beran A, Kahlon N, Hamouda D. Midostaurin in advanced systemic mastocytosis: a systematic review and meta-analysis. Am J Ther. 2022.
- Trujillo JA, Godfrey J, Hu Y, et al. Primary resistance to CD19-directed chimeric antigen receptor T-cell therapy in T-cell/histiocyte-rich large B-cell lymphoma. Blood. 2021; 137: 3454-3459.
- Kahlon N, Abuhelwa Z, Doddi S, Hamouda D. Post-cardiac arrest leukocytosis mimicking acute monocytic leukemia. Cureus. 2022; 14: e29508.
- Zheng SM, Zhou DJ, Chen YH, Jiang R, Wang YX, Zhang Y, Xue HL, Wang HQ, Mou D, Zeng WZ. Pancreatic T/histiocyte-rich large B-cell lymphoma: a case report and review of literature. World J Gastroenterol. 2017; 23: 4467-4472.
- Kahlon N, Baddam S, Bansal N, Qureshi Z, Maradana J. Dynamic changes in breast cancer receptor status: a case report highlighting the importance of repeat biopsies in guiding treatment strategies. J Investig Med High Impact Case Rep. 2025.
- Tamhane S, Menon LP, Edem D, Sharma P, Maradana J. Ectopic adrenocorticotropic hormone-producing metastatic gastrinoma: a case report. Cureus. 2023; 15: e45329.