
SciBase Journals
SciBase Clinical and Medical Case Reports
ISSN 2691-7785
- Article Type: Case Report
- Volume 3, Issue 1
- Received: Oct 08, 2025
- Accepted: Nov 20, 2025
- Published Online: Nov 27, 2025
Modified Gerwin Surgical Technique for Pediatric Proximal Humerus Osteochondroma: A Case Report
Mohamed Hamid Awadelseid*
Associate Professor of Pediatric Orthopedic Surgery, Excellence Trauma Centre Khartoum, Sudan.
*Corresponding Author: Mohamed Hamid Awadelseid
Associated Professor of Pediatrics Orthopedic Surgery, Excellence Trauma Centre Khartoum, Sudan.
Email: mhawad3055@gmail.com
Abstract
Introduction: The anterior and anterolateral approaches to the humerus describe splitting brachialis longitudinally, assuming its fibres run parallel to the shaft. A recent anatomic study has demonstrated the predictability of the position of the axillary nerve as it crosses the anterior deltoid raphe, which allows it to be isolated and protected, and dissection can be extended distally. In addition, no accessory motor branches to the anterior head of the deltoid cross the raphe, so extending an incision through the raphe after protecting the main motor branch of the axillary does not place the innervation to the anterior deltoid at risk. This the Modified Gerwin Approach allows exposure of the proximal humerus and indirect reduction of the fracture, with subsequent locking plate fixation, adhering to the principles of biological fixation.
Methods: Surgical Technique: Patient positioning: Supine or beach-chair position. Incision: Anterolateral incision (3-6 cm) between the deltoid and biceps muscles. Dissection: Interval between deltoid and biceps muscles developed. Retraction: Deltoid muscle retracted posteriorly; biceps muscle retracted anteriorly. Humerus exposure: Radial nerve and profunda brachii artery identified and protected. Procedure-specific steps: Perform fracture fixation, tumor resection, infection management, or neurological procedure.
Results: Advantages: Minimal muscle damage. Excellent visualization of proximal humerus. Reduced risk of radial nerve injury. Easy conversion to deltpectoral approach. Potential Complications: Radial nerve injury. Axillary artery damage. Infection. Fracture or hardware failure. Muscle weakness or atrophy.
Conclusions: Improved anatomical understanding: The Modified Gerwin Approach surgical exposure to the proximal humerus provides the largest humeral exposure with the greatest visibility of landmarks relative to the most widely utilized standard approaches. Minimal muscle damage with excellent visualization of proximal humerus and reduced risk of radial nerve injury and Easy conversion to deltpectoral approachs demonstrates satisfactory outcomes using this approach.
Keywords: Modified; Gerwin; Proximal; Humerus; Osteochondroma.
Citation: Awadelseid MH. Modified Gerwin Surgical Technique for Pediatric Proximal Humerus Osteochondroma: A Case Report. SciBase Clin Med Case Rep. 2025; 3(1): 1037.
Introduction
The deltopectoral surgical approach is most frequently used and requires significant muscle retraction and soft tissue stripping to expose the lateral humeral neck. This may contribute to avascular necrosis and fixation failure. Lateral approaches have been limited to 5 cm distal to the acromion because of the course of the anterior branch of the axillary nerve [1]. A recent anatomic study has demonstrated the predictability of the position of the axillary nerve as it crosses the anterior deltoid raphe, ISSN: 2995-5874 which allows it to be isolated and protected, and dissection can be extended distally. In addition, no accessory motor branches to the anterior head of the deltoid cross the raphe, so extending an incision through the raphe after protecting the main motor branch of the axillary does not place the innervation to the anterior deltoid at risk [2]. This the Modified Gerwin Approach allows exposure of the proximal humerus and indirect reduction of the fracture, with subsequent locking plate fixation, adhering to the principles of biological fixation [3].
Adequate exposure of the proximal humerus is necessary to address atypical or complex proximal humerus fractures and orthopedic tumors. Surgical management may be difficult through existing approaches due to their limited nature and the delicate neurovascular anatomy of the shoulder. the Modified Gerwin Approach, a previously described extensile approach, can be incorporated into the surgeon’s armamentarium as an alternative exposure to the proximal humerus [4].
The objective of this study was to quantify and compare the humeral exposure achieved through the Modified Gerwin Approach with the standard direct lateral deltoid-splitting, anterolateral acromial, and deltopectoral approaches in terms of surface area and exposure of key anatomic landmarks.
Indications the Modified Gerwin Approach
Proximal humerus fractures (e.g., two-part, three-part, four-part), Humeral head fractures and Proximal humerus nonunions or malunions also inTumor resections and Shoulder arthroplasty [5].
Methods
After identifying landmarks, exposure area of exposed humerus was quantified using digital images in Surgical Technique.
• Patient positioning: Beach-chair or supine position with arm abduction.
• Incision: Anterolateral incision (5-7 cm) between deltoid and biceps muscles (Figure 1).
• Dissection: Interval between deltoid and biceps developed (Figure 2).
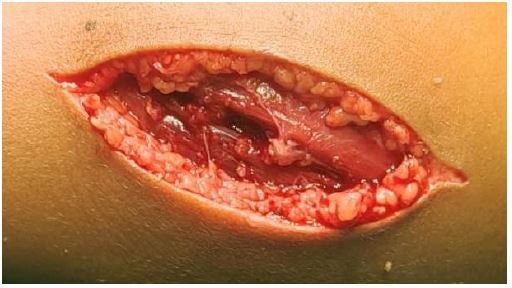
• Retraction: Deltoid muscle retracted posteriorly; biceps muscle retracted anteriorly (Figure 3).
• Proximal humerus exposure: Radial nerve and axillary artery identified and protected (Figure 4).
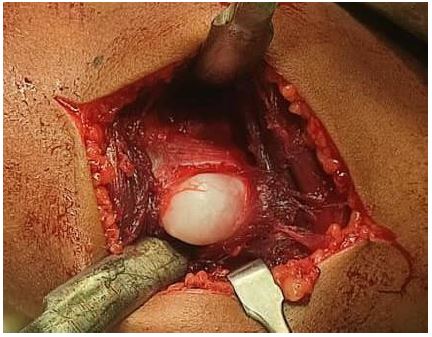
• Procedure-specific steps: Perform fracture reduction, fixation, or tumor resection close wound in layers (Figure 5) [6].
Results
After



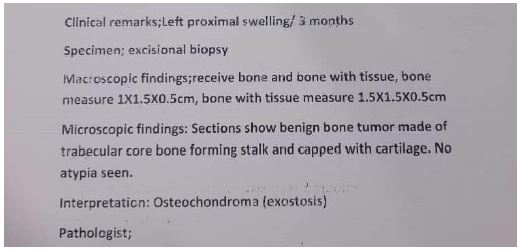
All anatomic landmarks were directly visible through the Modified Gerwin Approach as compared with the remaining approaches, through which only 1 landmark was directly visualized and only 2 of the 3 remaining were palpable through the approach and finally clinical pathology result with complete excision Figure [6].
Conclusion
The Modified Gerwin Approach surgical exposure to the proximal humerus provides the largest humeral exposure with the greatest visibility of landmarks relative to the most widely utilized standard approaches advantages minimal muscle damage, Excellent visualization of proximal humerus, Reduced risk of radial nerve injury and Easy conversion to deltpectoral approach [7].
Declarations
Consent: The authors confirm that informed consent was obtained from the patient for publication of this case report.
References
- Gerwin M, Hotchkiss RN, Weiland AJ. A surgical approach to the humerus. J Orthop Trauma. 1996; 10: 271–6.
- Jupiter JB, von Keudell A, Ring D. Surgical exposures of the upper extremity. J Orthop Trauma. 2017; 31: S1–8.
- Ring D, Perey BH, Jupiter JB. Surgical exposure of the proximal humerus. Tech Shoulder Elbow Surg. 2004; 5: 62–7.
- Jupiter JB, Ring D. Fractures and dislocations of the upper extremity. In: Bucholz RW, Heckman JD, Court-Brown CM, Tornetta P, editors. Rockwood and Green’s fractures in adults. 8th ed. Philadelphia: Wolters Kluwer. 2016: 843–56.
- Hoppenfeld S, DeBoer P. Surgical exposures in orthopaedics: the anatomic approach. 5th ed. Philadelphia: Wolters Kluwer. 2019.
- Orthobullets. Gerwin approach.
- AO Surgery Reference. Proximal humerus – Gerwin approach.