SciBase Journals
SciBase Critical Care and Emergency Medicine
- Article Type: Research Article
- Volume 2, Issue 3
- Received: Aug 05, 2024
- Accepted: Sep 20, 2024
- Published Online: Sep 27, 2024
The Impact of Platelets and their Derivatives on the Progression to Decompensation in Patients with Hepatitis B-Related Cirrhosis
Aylin Dolu Karaca1; Mehdi Karasu2*; Yücel Karaca2; Emin Bodakçı3; Nesibe Aydoğdu4; Yılmaz Bilgiç5
1Department of Rheumatology, Firat University Faculty of Medicine Elazig, Turkey.
2Department of Cardiology, Fethi Sekin Sehir Hastanesi, Elazig, Turkey.
3Department of Gastroenterology, Gaziantep Şehir Hastanesi, Gaziantep, Turkey.
4Department of Internal Medicine, Fethi Sekin Sehir Hastanesi, Elazig, Turkey.
5Department of Gastroenterology, Istanbul Medipol University, İstanbul, Turkey.
*Corresponding Author: Mehdi Karasu
Department of Cardiology, Fethi Sekin Sehir Hastanesi,
Elazig, Turkey.
Tel: +90-507-752-14 41;
Email: mehdikarasu@yahoo.com
Abstract
Background: Chronic Hepatitis B virus (HBV) infection often progresses to cirrhosis, which can lead to decompensation and increased morbidity. Predicting decompensation in HBV-related cirrhosis remains clinically challenging.
Objective: This retrospective study aimed to evaluate the utility of platelet count and its derivatives Mean Platelet Volume (MPV), Platelet Distribution Width (PDW), Plateletcrit (PCT) as markers for predicting decompensation in patients with HBVrelated cirrhosis.
Methods: Data were retrospectively collected from 131 patients diagnosed with HBV-related cirrhosis at İnönü University Turgut Özal Medical Center between January 2010 and December 2016. Patients were categorized into compensated (n=44) and decompensated (n=87) groups based on clinical manifestations (ascites, variceal bleeding, hepatic encephalopathy) and laboratory parameters (total bilirubin, International Normalized Ratio [INR]). Demographic, clinical, and laboratory data including platelet indices (PLT, MPV, PDW, PCT) were analyzed.
Results: There were no significant differences in platelet indices between compensated and decompensated groups. Elevated total bilirubin (p=0.008) and INR (p=0.015) levels were significantly associated with decompensated cirrhosis. Other hematologic and biochemical markers showed no significant differences between groups.
Conclusion: Platelet count and its derivatives (MPV, PDW, PCT) did not emerge as reliable predictors of decompensation in HBV-related cirrhosis. Elevated total bilirubin and INR levels were identified as significant markers of advanced liver dysfunction and decompensation. Future prospective studies with larger cohorts are needed to validate these findings and identify comprehensive predictors of decompensation in HBV-related cirrhosis.
Keywords: Hepatitis B-related cirrhosis; Decompensation; Platelet derivatives.
Citation: Karaca AD, Karasu M, Karaca Y, Bodakçı E, Aydogdu N, et al. The Impact of Platelets and their Derivatives on the Progression to Decompensation in Patients with Hepatitis B-Related Cirrhosis. SciBase Crit Care Emerg Med. 2024; 2(3): 1012.
Introduction
HBV is the most minor human-infecting Hepadnaviridae DNA virüs [1]. The WHO predicts 240 million HBV infections [2]. Twenty million Americans have had HBV, 3.5-4 million are carriers, and 500,000-1,000,000 have chronic HBV [3]. HBV infects hepatocytes, leading to asymptomatic carriers, acute or chronic hepatitis, liver cirrhosis, HCC, and other significant liver disorders [1]. Most individuals do not suffer hepatic problems, but 15-40% may develop significant sequelae [2].
Most chronic liver diseases end in cirrhosis with clinical decompensation [4]. 5-7% of compensated cirrhosis patients become decompensated after a few years. Decompensation means systemic cirrhosis. Decompensation causes ascites, variceal hemorrhage, hepatic encephalopathy, and icterus [5,6]. Grade and stage affect prognosis and treatment [4]. The transition to decompensated cirrhosis signifies a poor prognosis and necessitates urgent medical intervention.
Due to the complex history of HBV infection, biochemistry, viral serology, and disease staging are needed to manage and prognosticate HBV patients [7]. Biochemical markers such as ALT, AST, GGT (Gamma-Glutamyl Transferase), ALP (Alkaline Phosphatase), bilirubin, serum albumin and globulins, complete blood count, and prothrombin time should be measured to assess liver disease severity. HBV-related antigens and antibodies in patient serum distinguish between acute and chronic HBV infection, evaluate infectivity, investigate immune status, and screen blood and organ donors [8-10].
Chronic liver disease patients often develop thrombocytopenia (platelet count < 150,000 /μL). Moderate thrombocytopenia (platelet count, 50,000 /μL - 75,000 /μL) affects 13% of patients with cirrhosis. Many factors can cause thrombocytopenia, including splenic platelet sequestration, bone marrow suppression by chronic hepatitis C infection, and antiviral therapy with interferon-based therapy. A decrease in the level or activity of the hematopoietic growth factor thrombopoietin may also contribute.
Platelet count and its derivatives, such as Mean Platelet Volume (MPV), Platelet Distribution Width (PDW), and Plateletcrit (PCT), have been studied as potential markers of liver disease severity [11,12]. Thrombocytopenia, or low platelet count, is a common feature in cirrhosis due to hypersplenism, bone marrow suppression, and decreased thrombopoietin production. However, the role of platelets and their indices in predicting the transition from compensated to decompensated cirrhosis remains unclear.
This study aims to evaluate the usability of platelet count and its derivatives as markers in patients with Hepatitis B-related cirrhosis to identify early predictors of decompensation.
Materials and methods
This retrospective study was conducted at İnönü University Turgut Özal Medical Center and included patients diagnosed with Hepatitis B-related cirrhosis between January 2010 and December 2016. The study population comprised 131 patients who were divided into two groups: those with compensated cirrhosis and those with decompensated cirrhosis. The diagnosis of cirrhosis was confirmed through clinical evaluation, imaging studies, and, where necessary, liver biopsy.
Data collection: Data were retrospectively collected from electronic medical records. The following parameters were recorded for each patient:
Demographic data: Age and gender
Clinical data: Ascites grades [13], varicose grades [14], hepatic encephalopathy grades [15] and HCC +/-.
Laboratory data: Hemogram parameters including platelet count (PLT), Mean Platelet Volume (MPV), Platelet Distribution Width (PDW), PLATELETCRİt (PCT), Hemoglobin (HGB), White Blood Cell Count (WBC), and coagulation parameters (INR). Biochemical parameters including Alanine Aminotransferase (ALT), Aspartate Aminotransferase (AST), Blood Urea Nitrogen (BUN), creatinine, total protein, albumin, and total bilirubin.
Decompensated cirrhosis was defined by the presence of complications such as ascites, variceal bleeding, hepatic encephalopathy, or jaundice. According to the values of those with a corrected Child-Pugh score of 7 and above. The compensated group was divided into those with a CHILD score of 5 or 6 points and those without a decompensation clinic (Table 1).
Statistical analysis
The data for measurable variables were presented with the mean (minimum-maximum) and descriptive criteria test. Pearson Chi-Square analysis, Unpaired T test, Independent Samples Test, NPar Test, and Mann-Whitney Test were used to compare multiple data and detect differences. Values with p<0.05 were considered statistically significant.
Results
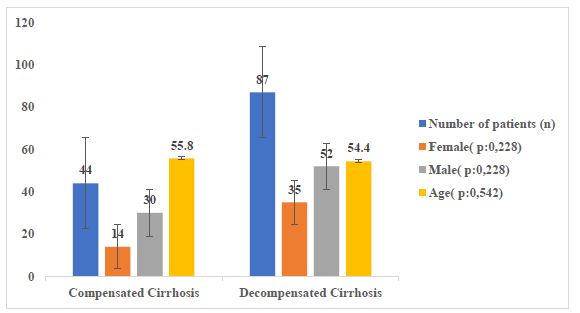
Of the 131 patients in the study, 44 had compensated cirrhosis, and 87 had decompensated cirrhosis. There was no significant difference between the patients with compensated cirrhosis in terms of gender, as 14 were female (32%), 30 were male (68%), 35 were female (40%), and 52 were male (60%) of the patients with decompensated cirrhosis. The mean age of the patients with compensated cirrhosis was 55.8 years, and the decompensated group was 54.4 years, and there was no significant difference between the two groups (Figure 1).
Table 1: Adjusted child-pugh classification [16].
| Parameters | 1 | 2 | 3 |
|---|---|---|---|
| Total SerumBilirubin Level | <2 mg/dL(34 μmol/L) | 2-3 mg/dL(35-51 μmol/L) | >3 mg/dL(>52 µmol/L) |
| Serum AlbuminLevel | >3.5 g/dL(35 g/dL) | 2.8-3.5 g/Dl(28-35 g/L) | <2.8 g/dL (<28 g/L) |
| International Normalized Ratio (prothrombin time) (INR) | <1.70 | 1.71-2.20 | >2.20 |
| Acid | None | Under control with mild or medical treatment | Severe or resistant to treatment |
| Hepatic Encephalopathy | None | Grade 1-2 or controlled by treatment | Grade 3-4 or refractory with treatment |
*Child A class: 5-6 points, Child B class: 7-9 points, Child C class: 10-15 points.
When patients are evaluated in terms of hemogram and biochemical markers, ALT (IU/L), AST (IU/L), BUN (mg/dL), Creatinine (mg/dl), WBC, MPV values are high in decompensated cirrhosis, while albumin (g/dL) HGB, PCT, PDW, PLT, Total Protein (mg/dL) values were high in compensated patients. However, the differences between the two groups were not statistically significant. Only total bilirubin (p:0.008) and INR (p:0.015) rates were significant (Table 2).
A significant difference was found when the patients in both groups were compared according to the degree of ascites and varicose.
Table 2: Comparison of hemogram and biochemical.
| Values | CompensatedCirrhosis | DecompensatedCirrhosis | pvalues |
|---|---|---|---|
| Albumin (g/dL) | 3,21±0,70 | 2,98±0,71 | 0,098 |
| ALT (IU/L) | 95,6±313,7 | 223±662,7 | 0,367 |
| AST (IU/L) | 321,1±1593 | 442±1430,5 | 0,105 |
| BUN (mg/dL) | 28,7±22,4 | 45,8±44,8 | 0,210 |
| Creatinine (mg/dl) | 1,49±1,49 | 2,13±4,47 | 0,966 |
| HGB | 11,8±2,92 | 10,9 ±2,67 | 0,078 |
| WBC | 7,22±5,02 | 7,42±5,97 | 0,821 |
| INR | 1,3±0,63 | 2,01±1,74 | 0,015* |
| MPV | 9,40±1,75 | 9,99±3,51 | 0,770 |
| PCT | 0,38±1,75 | 0,30±1,80 | 0,154 |
| PDW | 15,8±2,53 | 15,5±3,00 | 0,722 |
| PLT | 125,07±77,8 | 120,0±111,5 | 0,361 |
| Total bilirubin (mg/dL) | 3,16±4,96 | 5,83±7,52 | 0,008* |
| Total Protein (mg/dL) | 6,5±1,11 | 6,4±1,15 | 0,617 |
*Statistical significance was accepted when P- the value is < 0.05.
Table 3: Comparison of acid, varicose, and encephalopathy.
| Group | Grade 0 | Grade 1 | Grade 2 | Grade 3 | p-value | ||
|---|---|---|---|---|---|---|---|
| Acid | Compensated cirrhosis | 39 | 1 | 2 | 3 | 0,000 | |
| Decompensated cirrhosis | 9 | 16 | 27 | 35 | |||
| Varicose | Compensated cirrhosis | 33 | 3 | 5 | 3 | <0.05 | |
| Decompensated cirrhosis | 12 | 10 | 34 | 30 | |||
| Grade 0 | Grade 1 | Grade 2 | Grade 3 | Grade 4 | p-value | ||
| Encephalopathy | Compensated cirrhosis | 44 | 0 | 0 | 0 | 0 | 0,001 |
| Decompensated cirrhosis | 67 | 11 | 5 | 3 | 1 | ||
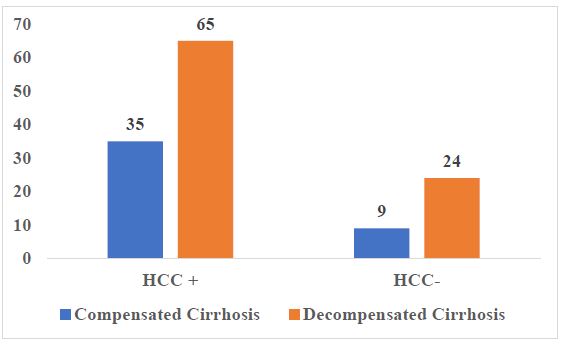
When the patients in both groups were evaluated in terms of HCC development, no statistically significant difference was found (p>0.05) (Figure 2).
Discussion
Cirrhosis represents the end stage of chronic liver disease, often resulting from persistent HBV infection. The transition from compensated to decompensated cirrhosis marks a significant decline in liver function and an increase in morbidity and mortality. Identifying reliable predictors for this transition is crucial for timely intervention and improved patient outcomes. Our study aimed to evaluate the utility of platelet count and its derivatives (MPV, PDW, and PCT) as potential markers for predicting decompensation in patients with HBV-related cirrhosis.
Our findings indicated no significant differences in platelet count, MPV, PDW, and PCT between patients with compensated and decompensated cirrhosis. These results suggest that platelet indices may not be reliable predictors of cirrhosis progression in HBV-infected individuals. However, our study identified elevated total bilirubin and INR levels as significant markers associated with decompensated cirrhosis, aligning with the existing literature on liver dysfunction.
Thrombocytopenia is common in patients with chronic liver diseases, including cirrhosis [17]. In the study of [18], three groups of patients, 40 with cirrhosis, 43 with cirrhosis and sepsis, and 61 healthy, were compared by comparing their PLT, MPV, PDW, and PCT values. PCT was significantly lower in the cirrhosis group than in the control group (0.09 vs. 0.22%, p-value< 0.05). Moreover, in this study, MPV and PDW were found to be significantly higher than the control population (17.83 vs. 16.56 fl, p-value<0.05) [18]. In our study, the compensated and decompensated groups exhibited thrombocytopenia, with median platelet counts falling below the normal reference range. However, our study found no significant associations between these parameters and decompensation in HBV-related cirrhosis patients.
Previous studies have yielded mixed results regarding the predictive value of platelet indices in liver disease. For instance, [19] reported that platelet count, when used in conjunction with spleen diameter, could predict the severity of liver fibrosis in patients with chronic hepatitis C. Conversely, other studies, such as those by [20], have found no significant association between platelet indices and liver disease severity in HBV-infected patients. These discrepancies highlight the variability in the utility of platelet indices across different etiologies of liver disease.
In contrast to our findings, some studies have reported that MPV and PDW can be useful in assessing the severity of liver fibrosis and cirrhosis [21] suggested that higher MPV levels were associated with more advanced fibrosis stages in chronic hepatitis B patients. However, these studies often involve different patient populations and methodologies, which may account for the variations in results.
In the study of [22] between 2006 and 2012, 203 patients with thrombocytopenia were examined by bone marrow biopsy. Of the patients, 179 (88%) had no known liver disease, and 12% had known liver disease. It was determined that 47 patients (25%) with thrombocytopenia who did not have liver disease before had cirrhosis [22].
The complex interplay between the liver, spleen, and bone marrow in cirrhosis may further complicate the relationship between platelet indices and disease severity. Hypersplenism, a common feature in cirrhosis, leads to platelet sequestration and destruction, while thrombopoietin production is impaired due to reduced liver function. These factors collectively contribute to thrombocytopenia, but their impact on MPV, PDW, and PCT remains unclear.
Our study’s identification of elevated total bilirubin and INR levels as markers of decompensation is consistent with previous research. For example, a study by Schuppan and Afdhal [23] found that elevated bilirubin and prolonged INR were significant predictors of liver disease progression and poor prognosis. These markers reflect the extent of hepatic dysfunction and impaired synthetic capacity, which are hallmarks of advanced liver disease.
The absence of significant findings related to platelet indices in our study could be attributed to several factors. The heterogeneity of the patient population, including the presence of coexisting conditions that may affect platelet parameters, could obscure potential associations. Additionally, the retrospective design of the study may limit the ability to capture dynamic changes in platelet indices over time. Future prospective studies with larger sample sizes and more homogeneous populations are necessary to validate these findings.
Our study has some limitations that should be acknowledged. Firstly, it was a retrospective study, and the data were collected from medical records, which may introduce inherent biases. Secondly, the sample size was relatively small, limiting the generalizability of the findings. Future prospective studies with larger sample sizes are warranted to validate these results further.
Conclusion
In conclusion, our study found no significant differences in platelet count, MPV, PDW, and PCT between compensated and decompensated HBV-related cirrhosis patients, suggesting that these indices alone may not be reliable predictors of decompensation. However, elevated total bilirubin and INR levels were significantly associated with decompensated cirrhosis, reaffirming their role as markers of advanced liver disease. Future studies should aim to identify a combination of markers that can accurately predict the transition to decompensated cirrhosis, thereby improving patient management and outcomes.
References
- Wu C C, Chen Y S, Cao L, Chen X W, Lu M J. Hepatitis B virus infection: Defective surface antigen expression and pathogenesis. In World Journal of Gastroenterology. 2018; 24(31). https://doi.org/10.3748/wjg.v24.i31.3488.
- Gish R G, Given B D, Lai C L, Locarnini S A, Lau J Y N, et al. Chronic hepatitis B: Virology, natural history, current management and a glimpse at future opportunities. In Antiviral Research. 2015; 121. https://doi.org/10.1016/j.antiviral.2015.06.008.
- Tozun N, Ozdogan O, Cakaloglu Y, Idilman R, Karasu Z, et al. Seroprevalence of hepatitis B and C virus infections and risk factors in Turkey: A fieldwork TURHEP study. Clinical Microbiology and Infection. 2015; 21(11). https://doi.org/10.1016/j.cmi.2015.06.028.
- Goodman Z D. Grading and staging systems for inflammation and fibrosis in chronic liver diseases. Journal of Hepatology. 2007; 47(4): 598-607. https://doi.org/10.1016/J.JHEP.2007.07.006.
- D’Amico G, Garcia-Tsao G, Pagliaro L. Natural history and prognostic indicators of survival in cirrhosis: A systematic review of 118 studies. In Journal of Hepatology. 2006; 44(1). https://doi.org/10.1016/j.jhep.2005.10.013.
- Merkel C, Bolognesi M, Angeli P, Noventa F, Caregaro L, et al. Prognostic Indicators of Survival in Patients with Cirrhosis and Esophageal Varices, without Previous Bleeding. The American Journal of Gastroenterology. 1989; 84(7). https://doi.org/10.1111/j.1572-0241.1989.tb02640.x.
- Qamar A A, Grace N D, Groszmann R J, Garcia-Tsao G, Bosch J, et al. Incidence, Prevalence, and Clinical Significance of Abnormal Hematologic Indices in Compensated Cirrhosis. Clinical Gastroenterology and Hepatology. 2009; 7(6). https://doi.org/10.1016/j.cgh.2009.02.021.
- Fattovich G, Brollo L, Giustina G, Noventa F, Pontisso P, et al. Natural history and prognostic factors for chronic hepatitis type B. Gut. 1991; 32(3). https://doi.org/10.1136/gut.32.3.294.
- Hadziyannis S J, Papatheodoridis G V. Hepatitis B e antigen-negative chronic hepatitis B: Natural history and treatment. In Seminars in Liver Disease. 2006; 26(2). https://doi.org/10.1055/s-2006-939751.
- Liu Yin J, Cussen C, Harrington C, Foskett P, Raja K, et al. Guideline Review: European Association for the Study of Liver (EASL) Clinical Practice Guidelines on Haemochromatosis. In Journal of Clinical and Experimental Hepatology. 2023; 13(4). https://doi.org/10.1016/j.jceh.2022.11.003.
- Ceylan B, Mete B, Fincanci M, Aslan T, Akkoyunlu Y, et al. A new model using platelet indices to predict liver fibrosis in patients with chronic hepatitis B infection. Wiener Klinische Wochenschrift. 2013; 125(15-16). https://doi.org/10.1007/s00508-013-0394-3.
- Pan Y, Muheremu A, Wu X, Liu J. Relationship between platelet parameters and hepatic pathology in patients with chronic hepatitis B infection - a retrospective cohort study of 677 patients. Journal of International Medical Research. 2016; 44(4). https://doi.org/10.1177/0300060516650076.
- Moore K P, Wong F, Gines P, Bernardi M, Ochs A, et al V. The management of ascites in cirrhosis: Report on the consensus conference of The International Ascites Club. Hepatology. 2003; 38(1). https://doi.org/10.1053/jhep.2003.50315.
- Wani Z A, Bhat R A, Bhadoria A S, Maiwall R, Choudhury A. Gastric varices: Classification, endoscopic and ultrasonographic management. In Journal of Research in Medical Sciences. 2015; 20(12). https://doi.org/10.4103/1735-1995.172990.
- Leise M D, Poterucha J J, Kamath P S, Kim W R. Management of Hepatic Encephalopathy in the Hospital. Mayo Clinic Proceedings. 2014; 89(2): 241-253. https://doi.org/10.1016/J.MAYOCP.2013.11.009.
- Şenaran H, Ileri M, AltinbaŞ A, KoŞar A, Yetkin E, et al. Thrombopoietin and mean platelet volume in coronary artery disease. Clinical Cardiology. 2001; 24(5): 405-408. https://doi.org/10.1002/CLC.4960240511.
- Alkhouri N, Morris-Stiff G, Campbell C, Lopez R, Tamimi T A R, et al. Neutrophil to lymphocyte ratio: A new marker for predicting steatohepatitis and fibrosis in patients with nonalcoholic fatty liver disease. Liver International. 2012; 32(2). https://doi.org/10.1111/j.1478-3231.2011.02639.x.
- Mukker P, Haridas A, Kallinkeel N, G A. Comparative study of platelet indices in cirrhosis, cirrhosis with sepsis and normal population. International Journal of Research in Medical Sciences. 2016. https://doi.org/10.18203/2320-6012.ijrms20161203.
- Giannini, Edoardo G, et al. Platelet count/spleen diameter ratio for the noninvasive diagnosis of esophageal varices: Results of a multicenter, prospective, validation study. Official journal of the American College of Gastroenterology| ACG. 2006; 101(11): 2511-2519.
- Morishita, Naoki, et al. Liver stiffness measurement by acoustic radiation force impulse is useful in predicting the presence of esophageal varices or high-risk esophageal varices among patients with HCV-related cirrhosis. Journal of gastroenterology. 2014; 49: 1175-1182.
- Zhou, Jin-Yong, et al. High hepatitis B virus load is associated with hepatocellular carcinomas development in Chinese chronic hepatitis B patients: A case control study. Virology journal. 2012; 9: 1-5.
- Sheikh MY, Raoufi R, Atla PR, Riaz M, Oberer C, et al. Prevalence of cirrhosis in patients with thrombocytopenia who receive bone marrow biopsy. Saudi Journal of Gastroenterology. 2012; 18(4). https://doi.org/10.4103/1319-3767.98431
- Schuppan D, Afdhal N H. Liver cirrhosis. The Lancet. 2008; 371(9615): 838-851.