SciBase Journals
SciBase Critical Care and Emergency Medicine
- Article Type: Case Report
- Volume 2, Issue 3
- Received: Sep 09, 2024
- Accepted: Oct 16, 2024
- Published Online: Oct 23, 2024
Pre-Flight Pericardiocentesis Prior to Aeromedical Transportation in a Patient with Cardiac Tamponade: Case Report
Supinya Wannachotphawet; Boriboon Chenthanakij*; Krongkarn Sutham; Pavita Laohakul
Faculty of Medicine, Chiang Mai University, 110 Intawaroros Road, Si Phum, Muang, Chiang Mai 50200, Thailand.
*Corresponding Author: Boriboon Chenthanakij
Faculty of Medicine, Chiang Mai University, 110 Intawaroros Road, Si Phum, Muang, Chiang Mai 50200, Thailand.
Email: ws.supinya@gmail.com
Abstract
Background: Cardiac tamponade is the decompensated phase of cardiac compression from intrapericardial fluid pressure. When the hemodynamic is compromised, an intervention such as pericardiocentesis is required. In a primarily rural region where urgent procedures are unavailable, and the duration of ground transportation is not compatible, aeromedical transportation may play an important role. Pre-flight stabilization of the patient is highly important for a safe transfer and preventing clinical deterioration or even death during the evacuation.
Case presentation: An elderly male, with a history of chronic obstructive pulmonary disease (COPD) presented with shortness of breath and wheezing at a primary care in a rural, mountainous region in the North of Thailand. After nebulized relievers were given, his shortness of breath did not improve, and he developed an epigastric pain radiating to the right scapular. The patient was diagnosed early with cardiac tamponade using bedside Point-Of-Care Cardiac Ultrasound (POCUS). The patient shortly began to have an acute respiratory failure and alteration of consciousness. Although the normal range blood pressure was maintained by fluid resuscitation, tachycardia was persistent. The attending physician decided that a 3-hour ground transportation might not be safe for the patient, as a result, Sky Doctor, the emergency aeromedical service team of Thailand was activated. The decision to perform pre-flight pericardiocentesis was made. Two emergency physicians flew in with equipment to perform the procedure at the primary care, leading to a safe transfer of the patient by a helicopter to a tertiary hospital and patient survival to hospital discharge.
Conclusion: We present this case report to highlight the successful decision to perform pre-flight pericardiocentesis for the stability of the patient with cardiac tamponade and a safe transfer by a helicopter. Also, to emphasize the importance of the hands-on opportunity of POCUS skills in medical school which results in rapid diagnosis and resuscitation by a general physician in primary care, as well as patient survival in this case.
Keywords: Cardiac tamponade; Aeromedical transportation; Pericardiocentesis; Pre-flight intervention; POCUS.
Citation: Wannachotphawet S, Chenthanakij B, Sutham K, Laohakul P. Pre-Flight Pericardiocentesis Prior to Aeromedical Transportation in a Patient with Cardiac Tamponade: Case Report. SciBase Crit Care Emerg Med. 2024; 2(3): 1014.
Background
Cardiac tamponade is a medical emergency that results from an accumulation of pericardial fluid compressing the cardiac chambers, leading to impaired cardiac filling (reduction of preload), a decrease in cardiac output, hemodynamic compromise shock and death. There are several etiologies of pericardial accumulation such as hemorrhage from a penetrating wound to the heart, ventricular wall rupture from myocardial infarction, inflammatory or autoimmune diseases and metastatic tumor invading the pericardium. Cardiac tamponade has a strong association with worse in-hospital outcomes and mortality. Though rare, early recognition is imperative to reduce the incidence of death [1,2]. Cardiac tamponade can be deceptively difficult to diagnose as the body compensates for the hemodynamic effects by various mechanisms. The classic finding of Beck’s triad of muffled heart sounds, hypotension, and distended neck veins is present in less than 10% of cases [3]. When there is a hemodynamic compromise, pericardiocentesis is indicated as an emergency procedure. Though, given the invasiveness of pericardiocentesis, the rareness of the condition and limited experience of an available provider in performing the procedure, medical decision making at a primary care setting is crucial for patient survival. Northern Thailand is a mountainous region where ground transportation can be challenging for some local primary cares to a secondary or tertiary hospital where specialists and advanced procedures are available. Northern Thai Sky Doctor, the emergency aeromedical service of Northern Thailand was founded in 2009 to allow the opportunity to secure essential medical treatment for a severe illness or injury requiring medical intervention and advanced multidisciplinary teams that are locally unavailable or inadequate. Prior to evacuation, the impact of physiologic changes that can occur at higher altitudes must be considered. Patient homeostasis may need to be addressed to ensure patient safety and a safe transfer [4].
Case presentation
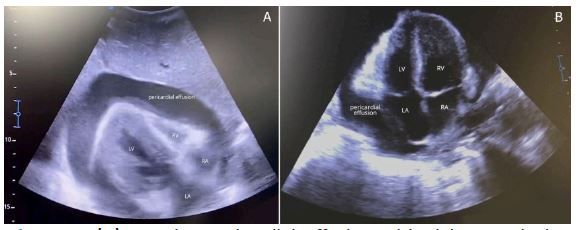
This case took place in a 30 beds primary, community hospital in rural area of Northern Thailand, located behind steep mountains, 137 kilometers away by ground from the closest tertiary hospital. A 72-year-old male patient with an underlying medical condition of Chronic Obstructive Pulmonary Disease (COPD) and history of exacerbations presented the emergency department with shortness of breath and wheezing an hour prior to the visit. Fenoterol/Ipratropium inhaler was tried at home but did not relieve the symptoms. There were also 5 times of diarrhea one night before. Initial vitals were as follows: Body Temperature: 36.6 c; Heart Rate: 127 bpm; Blood Pressure: 123/79 mmHg; Respiratory Rate of 32/minute, Arterial oxygen saturation on pulse oximeter of 95% without oxygen support. The patient looked fatigued. His consciousness was fully intact. There was dyspnea with increased respiratory effort and accessory muscles use. The air entry was poor and there was wheezing in both lungs on auscultation. There was no cyanosis, no edema, no visible neck vein engorgement. Only tachycardia was found. Distant heart sound was not suspected due to the loud emergency department setting. The patient was first diagnosed with COPD with exacerbation due to his presentation and underlying medical condition. Two doses of Fenoterol/Ipratropium via nebulizer were given, 15 minutes apart. After nebulization, the breath sound was clear and equal on both lungs. However, tachycardia and tachypnea did not improve. The patient suddenly began to complain of a new onset palpitation and epigastric discomfort radiating to the right scapular. Cardiac causes of shortness of breath and epigastric discomfort were suspected. 12 leads ECG and Chest x-ray was ordered and done shortly after. Bedside-POCUS was done immediately to evaluate the cause and to assess volume status for management decisions. The 3C-A convex ultrasonic transducer of the Sonoscape E2 model portable ultrasound machine was used by W.Supinya, M.D., a general physician with two months of experience as a licensed physician. The first view done was Inferior vena cava (IVC) view. Extremely large IVC was detected, following with a subxiphoid view that illustrated massive pericardial effusion with totally collapsed right ventricle (Figure 1). The 12-leads ECG showed sinus tachycardia of rate 131 bpm, with low voltage and electrical alternans. No ST-T change or T wave inversion was found. Chest radiographs demonstrated cardiomegaly which had significantly enlarged from previous film taken 4 months prior to this visit, before he lost the follow up, supporting the diagnosis of massive pericardial effusion (Figure 2). Right upper lung mass was seen and had expanded in size. Two large bore IVs were accessed and 1000 ml of 0.9% NaCl began to be loaded. Minutes after, respiratory effort was continuously increasing. The patient began to have an acute respiratory failure and deteriorated in consciousness to a drowsy stage. An endotracheal tube was successfully placed on the first attempt after the patient was sedated with 10 mg of diazepam IV. The patient was supported on a ventilator with minimal Positive End-Expiratory Pressure (PEEP). The regular system of consulting an emergency physician at a tertiary-level hospital was activated by phone to make patient referral. The case was accepted to be transferred via ground ambulance with the suggestion of IV fluid loading to maintain normal blood pressure or inotropic agent if needed. During the resuscitation and preparation of the referral team, the patient’s vitals became unstable. Blood pressure fluctuated between unmeasurable and around 60/35 mmHg. After the first liter of 0.9% NaCl was completely loaded, the blood pressure had improved to approximately 123/99 mmHg. Inotropic agents were not required to maintain normal range blood pressure. Yet, the pulse rate remained at 140-150 bpm even after the 2nd liter of fluid was given. The physician decided that the patient was not stable enough to be transferred by ground transportation which takes approximately 2.5-3 hours. The decision to activate Sky Doctor, the emergency aeromedical team, was made. The Sky Doctor team decided to fly to the rural hospital and perform pre-flight pericardiocentesis prior to aeromedical transportation by helicopter. The one-bed emergency room in this rural hospital was organized to become a small operating room. A double lumen catheter was brought from the tertiary center by the SkyDoctor team.
The patient was placed in supine position. The point of maximal effusion was identified using the cardiac probe. The right ventricle was found to have totally collapsed. The distance from skin surface to the effusion border was measured for expected needle depth. The sterile preparation was done with povidone-iodine and sterile draping. The cardiac probe of the portable ultrasound was placed in a sterile glove with gel on the probe tip. Pericardiocentesis was successfully performed under real-time ultrasound guidance using subxiphoid approach by two experienced emergency physicians. The double lumen catheter was placed, and 400 ml of fresh blood was drawn out of the pericardium. Ultrasound showed the restored right ventricular filling capacity and significantly better cardiac output. (Figure 1) After the procedure, the catheter was retained and sutured for possible further fluid release. The pulse rate suddenly improved to around 114 bpm. The blood pressure was stable at approximately 131/95 mmHg. The patient had gained back his consciousness before being transferred. The patient was safely evacuated. The attending cardiologist had the pericardial effusion drainage done daily in admission. Whole chest and abdomen CT scan illustrated a 4.5 x 4.0 x 4.9 cm heterogeneous enhancing mass in apical segment of right upper lung with multiple lymphatic metastasis. Primary lung cancer was first considered. He was discharged from the hospital without any cardio-respiratory support and neurologically intact after 11 days of admission. He came back for a follow up in the next two weeks with his family to have a discussion with an oncologist. He decided to deny any further invasive treatment at the tertiary center. Instead, palliative care at the initial local hospital in his hometown was planned for his best quality of life, for him to be at home when the last moment comes, and to be surrounded by his family members who all live in the same village. He lived to 31 days after the diagnosis with best possible support.
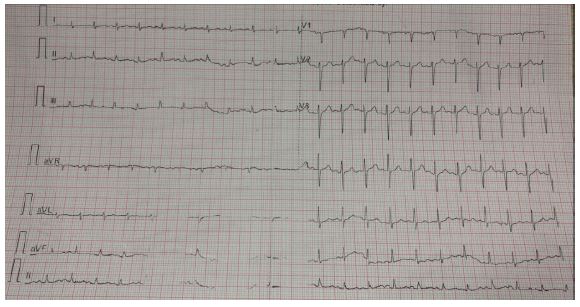
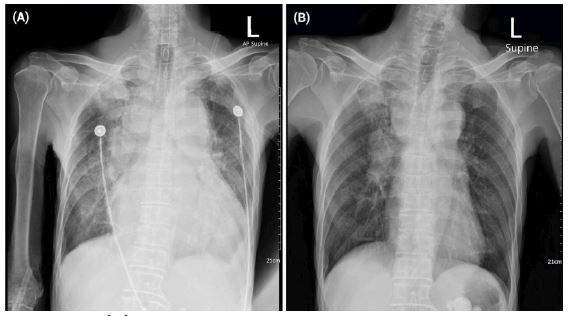
Discussion
A patient with a history of COPD presenting at an emergency department with shortness of breath and wheezing is a very common scenario seen especially in this region of the country where heavy homemade-tobacco smoking is a cultural behavior among hill tribe communities. Regardless of the previous and chronic respiratory problems, other causes of dyspnea should always be assessed. Especially in this case when the nebulized reliever did not improve the symptoms. Epigastric pain radiating to the back was another important sign that a cardiac cause of shortness of breath should be evaluated. Bedside ultrasound can be done immediately if available and is able to detect emergency, life threatening conditions such as cardiac tamponade in case, or other diagnosis such as myocardial infarction or aortic dissection. Without bedside ultrasound, cardiac tamponade can be deceptively difficult to diagnose as the body offsets for the hemodynamic effects by various mechanisms. The reduction of preload due to pericardial fluid pressure and the impaired cardiac output are compensated by the increase in heart rate and the increase in afterload by elevating the systemic vascular resistance [5]. Often, the only clinical finding of pericardial tamponade is sinus tachycardia. The classic finding of Beck’s triad of distant heart sounds, hypotension, and neck veins engorgement is present in less than 10% of cases [3,6]. In severe cases, one may note low voltage and electrical alternans in ECG. Chest radiographs may show cardiomegaly and may suggest pericardial effusion if a prior chest radiograph with a normal cardiac silhouette is available for comparison [7]. Cardiac tamponade can easily be missed and also has a strong association with worse in-hospital outcomes and mortality [8]. Early suspicion by the first attending physician at the primary care was crucial in this case for the patient’s chance of survival. Hypotension may be a sign of ominous decompensation and an emergent need for surgical intervention. According to the invasiveness of the pericardiocentesis, the rareness of the condition and limited experience of an available provider in performing the procedure, initial resuscitation was correctly done with an immediate decision making to activate the aeromedical team with a well understanding of the hospital context and limitations. The resuscitation was well managed at the primary care while waiting for the advanced team to come. The decision to wait for experienced personnel to arrive and perform pericardiocentesis was considered safe as the patient could be temporarily stabilized. Volume resuscitation, the initial resuscitation for cardiac tamponade was done. An inotropic agent was not given as the blood pressure could be maintained after IV fluid loading. As the patient developed an acute respiratory failure, airway management was properly done with endotracheal tube insertion with a mechanical ventilator support. Although positive pressure mechanical ventilation should be avoided in cardiac tamponade as it may further decrease venous return and aggravate the symptoms, the patient could not maintain adequate ventilation and might not be able to await the coming rescue. Airway management done with minimal PEEP and close monitoring was proper. Considering a chance of patient deterioration in a short period of time due to the severity of cardiac tamponade, persistent tachycardia regardless of the initial resuscitation and the impact of physiologic changes that can occur at higher altitudes, the patient’s homeostasis was needed to be addressed to ensure patient safety, better outcome, and a safe transfer. The Sky Doctor team decided to improve the patient’s condition and stabilize the vitals by flying to the rural hospital to perform pre-flight pericardiocentesis prior to aeromedical transportation by a helicopter. The successful pericardiocentesis resulted in a dramatic increase in cardiac output and blood pressure evidenced by an improvement in right ventricle collapse and the patient’s vital signs. The rapid and thorough clinical decision making, as well as the lifesaving procedure performed led to great outcomes for the patient after the rescue. In rural or small hospital settings with limited resources, the benefits of a portable ultrasound for life-threatening condition detection and lifesaving management can be significant [9,10]. This report also emphasizes the importance of basic POCUS training in general physician education level. This case was diagnosed by a general physician with two months of practical experience. The attending physician graduated from the faculty of medicine, Chiang Mai university which POCUS was first introduced into the curriculum in 2014. Multiple hand-on workshops and simulations of life-threatening emergency conditions with experienced professors in medical school helped prepare the physician to be able to detect, resuscitate and make clinical decisions for this case safely. As a result, we would like to encourage that having hands-on POCUS skill training in undergraduate medical school curriculum and creating opportunities for graduated general physicians to attend might positively impact the survival of patients in primary hospital settings.
Declarations
Acknowledgement: The authors are truly grateful and would like to thank Krittapas Thepprakarn, M.D. and Wiang Haeng hospital team who worked together to save the patient’s life. Also, thank you Chenthanakit B, Laohakul P, and the District 1 Emergency Aeromedical Service of the National Institute for Emergency Medicine of Thailand who performed pericardiocentesis and transferred the patient safely to tertiary care. Special thanks for Chenthanakit B, and Sutham K, for being the research advisers and supporters
Consent for publication: Written consent was obtained from the patient and the patient’s relative for publication of this case report and accompanying images.
Conflict of interests: The authors declare that they have no competing interests.
Ethics Approval: This study was approved by the chairman of the subcommittee of ethics of human research, Faculty of Medicine, Chiang Mai University, EME-2567-0041, Nakornping Hospital No.072/67
References
- Adler Y, Charron P, Imazio M, Badano L, Barón-Esquivias G, et al. ESC Guidelines for the diagnosis and management of pericardial diseases. Russ J Cardiol. 2016; (5): 117-62.
- Spodick DH. Acute cardiac tamponade. N Engl J Med. 2003; 349(7): 684-90.
- Ross C, Schwab T. Cardiac Trauma. In: Tintinalli JE, Stapczynski JS, Ma OJ, Yealy DM, Meckler GD, Cline DM, editors. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8e. New York, NY: McGraw-Hill Education. 2016. accessemergencymedicine.mhmedical.com/content.aspx?aid=1121495563
- Kamolchanok Boonsri, Krongkarn Sutham, Jamjuree Lerdjan, Srichai Klanarong, Thoranee Kayee, et al. District 1 Emergency Aeromedical Service committee of the National Institute for Emergency Medicine of Thailand. Emergency Aeromedical Service Guidance revision. 2014; 2014: 5-60.
- Fowler NO. Cardiac tamponade. A clinical or an echocardiographic diagnosis? Circulation. 1993; 87(5): 1738-41.
- Beck cs. Two cardiac compression triads. J Am Med Assoc. 1935; 104(9): 714-6.
- Electrical Alternans with Pericardial Tamponade NEJM 2023. https://www.nejm.org/doi/pdf/10.1056/NEJMicm1408805.
- Mehta RH, Suzuki T, Hagan PG, Bossone E, Gilon D, et al. Predicting death in patients with acute type A aortic dissection. Circulation. 2002; 105(2): 200-6.
- Murali S, Miller C, Zohn S, Yang B, Krebs W. Helicopter Emergency Medical Services Ultrasound Use in the Diagnosis of Pericardial Effusion Due to Aortic Dissection. Air Med J. 2022; 41(6): 566-9.
- Kaniecki DM. Pericardiocentesis in an ambulance: a case report and lessons learned. Air Med J. 2019; 38(5): 382-5.