SciBase Journals
SciBase Dentistry and Oral Sciences
ISSN 2691-7785
- Article Type: Short Commentary
- Volume 1, Issue 1
- Received: Oct 28, 2023
- Accepted: Dec 05, 2023
- Published Online: Dec 12, 2023
Comparison of Mandibular Morphology in Adult Patients with Unoperated Complete Bilateral Cleft Lip and Palate and Normal Subjects
Mohammad Sadegh Nazari1; Gholamreza Heidari1*; Leila Bazvand2
1Assistant Professor of Dentistry, Department of Orthodontics, School of Dentistry, Lorestan University of Medical Science, Iran.
2Endodontics Specialist, Department of Endodontics, Lorestan University of Medical Science, Iran.
*Corresponding Author: Gholamreza Haidari
Assistant Professor, Department of Orthodontics, School of Dentistry, Lorestan University of Medical Science, Khorramabad, Iran.
Email: ghrh61@yahoo.com
Abstract
Background and aim: Patients with Bilateral Cleft Lip and Palate (BCLP) are commonly recognized with abnormalities in craniofacial features that require orthodontic treatment to treat these abnormalities. Understanding the craniofacial development and development of these patients in different stages of treatment is important. The aim of this study was to evaluate the morphological characteristics of mandible in adults with complete bilateral cleft lip and palate and compare these features with normal subjects.
Materials and methods: The lateral cephalogram of 30 adults with mean age of 20±0.2 years, referring to orthodontics department of Tehran University of Medical Sciences (including 15 untreated non-syndromic BCL Pand 15 skeletal class l pattern patients with no cleft or other facial deformities). Anatomical landmarks were identified by one orthodontist and one operator and craniofacial parameters were measured twice by the operator. Data were analyzed using colmogorov-smirnov test and parameter comparison between two groups of BCLP and control group was performed using sample t-test. P<0.05 was considered significant.
Results: Gonial angle (P=0.004), mandibular plane angle (P=0.001) and Pog-N. perp distance (P=0.019) were significantly higher in BCLP group than control group. Ba.Na.Go angle (P=0.039), Facial angle (P=0.001), Ramus length (P=0.022) and Jarabak index (P=0.016) were significantly lower in the BCLP group than in the control group. Other variables including SNB angle, S.N.Pog angle, (N.S.Gn) Y-axis, mandibular body length, S-Go and N-Me showed no significant difference in BCLP group compared to control group.
Conclusions: According to the results of this study, it can be stated that the morphological characteristics that patients with bilateral cleft lip and palate are known to include: tendency for vertical facial growth, obtuse gonial angle, decrease ramus length, increased mandibular plane angle and chin retrusion. It can also be concluded that the morphologic features of the mandible in these patients can be considered as part of the abnormality and not merely as a result of the surgical treatments they have received.
Keywords: Untreated bilateral cleft lip and palate; Mandibular morphology; Adults.
Citation: Nazari MS, Heidari G, Bazvand L. Comparison of Mandibular Morphology in Adult Patients with Unoperated Complete Bilateral Cleft Lip and Palate and Normal Subjects. SciBase Dent Oral Sci. 2023; 1(1): 1003.
Introduction
Cleft lip and palate are the most common congenital craniofacial malformations, accounting for about 15% of all congenital malformations [1]. Thus, out of every 10,000 babies born in the United States, 7.75 have a cleft lip and palate, which is estimated at 7.94 per live birth for the rest of the world [2]. In Iran, there have been several studies of the incidence of cleft palate and lip andthe highest statistics were reported by Dr. Taheri et al. from 1983 to 1998 at Najmeh Hospital. This study found that 3.73 out of every 1,000 live births had cleft lip malformationswith or without cleft palate- which is a very high figure [3]. High prevalence of this anomaly was reported in Asian populations (0.374%-0.079%), moderate prevalence in white population (0.269-0.091%) and lower prevalence in African populations (0.167-0.018%) [4].
Various genetic and environmental factors affect the incidence of these lesions so that the etiology of them is multifactorial, environmental factors such as mother’s hormonal disorders, consumption of vitamins and folic acid, obesity and weight gain of mother, hypoxia and smoking and even the effect of season on prevalence were reported [5]. Hereditary factors such as race and ethnicity and some genes and even geographical areas and gender are also implicated in the occurrence of these anomalies [6].
Patients with cleft palate and lip are generally known to have Anomalies in the shape of the dental arch, malocclusions and craniofacial deformities, which require orthodontic treatment to treat these anomalies [7]. Understanding the development and evolution of patients with cleft lip and palate is important in the stages of diagnosis, treatment plan and prognosis. This is also important for other specialists who treat these patients [8].
During infancy and before surgery,craniofacial morphological features of cleft patients include protruded premaxilla, retrudedposition of maxilla, and decreased posterior maxillary height. Also in these newborns, the mandible is deficient and retruded, the prelibium lacks any muscle fibers, the nostrils are more elongated and the tip of nose is wider, the columella is shorter or absent, and the prelibium is attached directly to the nose. However, this subtype of cleft patients exhibits a variety of anatomy [9].
Many studies have been done on the facial morphological features of cleft palate and lip patient butthe results are different and sometimes contradictory [10,11]. The reason for these differences and inconsistencies is the differences in the treatment process for these patients, the different function of these patients due to the presence of clefts, as well as differences in their hereditary growth patterns [2].
The abnormal facial morphology in treated cleft lip and palate patients is influenced by two factors: 1) the nature of the disease (type of cleft) and 2) the type of treatment performed for these patients. Therefore examining untreated adult patients with cleft lips and palate helps us to exclude the impact of the type and number of surgical treatments and to examine only the morphological features resulting from this abnormality [1].
So the aim of this study is to investigate the morphological features of mandible in adults with untreated complete bilateral cleft lip and palate and compare these features with those without cleft.
Materials and methods
This retrospective study evaluated lateral cephalograms of 30 adult patients from Iran, Tehran University of Medical Sciences, orthodontic department. The patients were classified into 2 groups: 15 individuals with un operated complete Bilateral Cleft Lip and Palate (BCLP) and 15 individuals with no cleft. BCLP patients were ranging in age of 16 to 24 years. The inclusion criteria were availability of lateral cephalogram, surgical correction of the cleft in infancy (primary lip correction within 3-5 months and primary palate correction before 1 year), age of 15 years or more and no history of orthognathic surgery [1]. Also patients younger than 15 years and those with incomplete records, craniofacial fractures, tooth losses that could alter the vertical dimension and syndromic cases of CLP were excluded from the study [1,2].
The noncleft patients were also ranging in age of 16 to 24 years. The control group had normal craniofacial morphology, angle skeletal class Ι relationship, no history of functional therapy, orthognathic surgery or any jaw deformities.
BCLP and noncleft groups had no significant difference in age (p=0.33). The lateral cephalograms were taken as part of orthodontic treatment, so patients were not unnecessarily exposed to additional radiation. The lateral cephalograms were taken for the BCLP patients and the normal controls at one radiology clinic (dentistry faculty of Tehran university of medical sciences; radiology department), while FH plane parallel to the floor, teeth in centric occlusion and lips lightly in contact. The machine was calibrated for 60-70 kVp tube voltage, 10-14 mA tube current, and 16-second exposure time. Soft tissue and bony structures were traced on acetate cellulose papers, and the mean shadow of bilateral structures was traced to minimize slight errors.
Landmarks were identified by two person (one orthodontist and one operator).
The following landmarks were identified on each cephalogram (Figure 1):
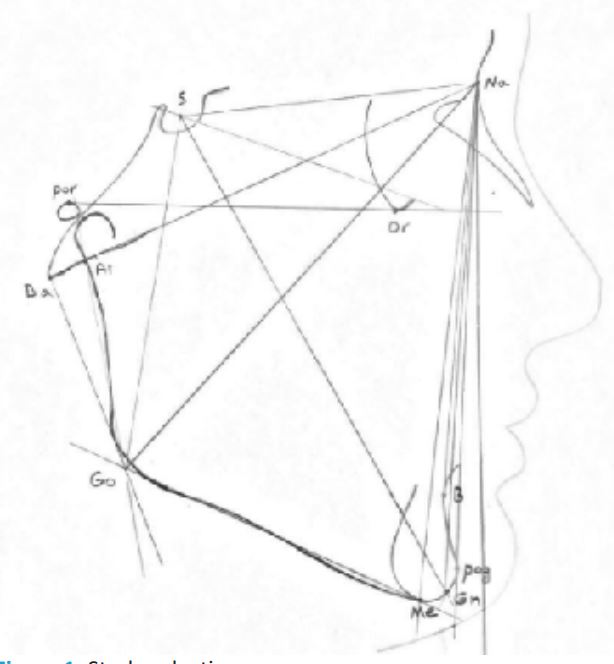
• B point (B), Basion (Ba), Gnathion (Gn), Gonion (Go), Menton (Me), Nasion (Na), Orbitale (Or), Pogonion (Pog), Porion (Por), and Sella (S).
The following angular and linear measurements were used in this study: Ar.Go.Me(ᵒ), S.N.B (ᵒ), S.N.Pog (ᵒ), N.S.Gn (ᵒ), Ba.Na.Go (ᵒ), SN to mandibular plane (ᵒ).
Pog to Na perpendicular (mm) (the distance from Pog to a line through nasion that is perpendicular to the Frankfort horizontal), Ar-Go (mm), Go-Me (mm), S-Go (mm), N-Me (mm) and jarabak index.
All statistical analyses were performed using SPSS version 22. Normality of the data was tested using the Kolmogorov-Smirnov test. All the data were analyzed statistically and mean values for each parameter in both groups were compared using sample t-test. P<0.05 was considered statistically significant.
Results
Table 1 shows parameters related to vertical dimension and Table 2 shows parameters related to sagittal dimension.
Table 1: Comparison of parameters in vertical dimension between control and BCLP groups.
| Control | BCLP | Mean diff | p.value | |||
|---|---|---|---|---|---|---|
| Parameter | Mean | SD | Mean | SD | ||
| Gonial.angle (degrees) | 120.66 | 7.79 | 131.93 | 11.49 | 11.26 | 0.004 |
| Ba.Na.Go (degrees) | 98.73 | 7.33 | 92.06 | 9.40 | -6.66 | 0.039 |
| SN.MP.angle (degrees) | 28.40 | 6.95 | 37.43 | 6.74 | 9.03 | 0.001 |
| Ramus.length (mm) | 63.83 | 6.83 | 57.03 | 8.39 | -6.80 | 0.022 |
| S.Go (mm) | 80.93 | 7.04 | 79.53 | 9.17 | -1.40 | 0.643 |
| N.Me (mm) | 118.03 | 8.46 | 124.70 | 11.89 | 6.66 | 0.088 |
| Jarabak.index | 68.67 | 5.22 | 63.79 | 5.23 | -4.87 | 0.016 |
| y.axis (degrees) | 68.43 | 3.99 | 69.66 | 5.89 | 1.23 | 0.508 |
Table 2: Comparison of parameters in sagittal dimension between control and BCLP groups.
| Control | BCLP | Mean diff | p.value | |||
|---|---|---|---|---|---|---|
| Parameter | Mean | SD | Mean | SD | ||
| SNB (degrees) | 78.53 | 3.54 | 77.96 | 4.39 | -0.56 | 0.700 |
| SN.Pog (degrees) | 79.20 | 4.31 | 79.13 | 4.67 | -0.06 | 0.968 |
| Facial.angle (degrees) | 89.56 | 2.61 | 85.16 | 4.06 | -4.40 | 0.001 |
| Pog.Nprep (mm) | 4.50 | 4.86 | 11.70 | 10.06 | 7.20 | 0.019 |
| Mand.body.length (mm) | 74.70 | 6.21 | 75.80 | 7.78 | 1.10 | 0.672 |
| N.Me (mm) | 118.03 | 8.46 | 124.70 | 11.89 | 6.66 | 0.088 |
| Jarabak.index | 68.67 | 5.22 | 63.79 | 5.23 | -4.87 | 0.016 |
| y.axis (degrees) | 68.43 | 3.99 | 69.66 | 5.89 | 1.23 | 0.508 |
The Gonial angle was significantly greater in BCLP group than in the control group (P=0.004). SN-MP angle was also significantly greater in BCLP group than in the control group (P=0.001). There was a significant difference in the Jarabak index between the BCLP group and the control group (P=0.016), indicating vertical pattern of growth in BCLP patients. Pog-n. perp distance was significanty greater in BCLP group than in the control group (P=0.019). Ba.Na.Go angle was significantly lower in BCLP group than in the control group (P=0.039). Facial angle (S.N.Gn) was significantly lower in BCLP group than in the control group (P=0.001). Ramus length (Ar-Go) was also significantly lower in BCLP group than in the control group (P=0.022). Statistical analysis didn’t find a significant difference in the other measured parameters between the two groups (P>0.05).
Discussion
In this study, some mandibular morphologic features of BCLP patients showed significant differences with those of non-cleft patients;
1) Vertical dimension:
Craniofacial growth pattern showed a tendency to vertical growth in BCLP patients.
• Mandibular plane angle was increased in BCLP patients for 9.03 mm than the control group.
• Gonial angle was also increased in BCLP patients for 11.27° than the control group.
• Jarabak index was decreased in BCLP patients for 4.88% than the control group.
These three parameter changes show the tendency to vertical growth in BCLP patients. These results are in agreement with the results reported in Silva Filho, Capelozza junior and Shetye studies [2,4,9].
The increased mandibular plane angle in BCLP patients could represent a clockwiase rotation of mandible in this group that also shows itself in the increased gonial angle and the decreased ramus length.
• Facial heights evaluated in our study were S-Go and N-Me that showed no significant difference with control group. This is in agreement with results reported in Silva Filho study [9].
• Ramus length was significantly shorter in BCLP patients than the control group and mandibular body length showed no significant difference between the two groups.
Other studies evaluating mandibular size in BCLP patients have measured mandibular effective length (Co-Gn). And all of them have reported decrease in mandibular effective length [2,4,9].
• Y-axis (N.S.Gn) showed no significant difference between the BCLP and control groups. And this is in agreement with Jahanbin study results [1].
• Ba.Na.Go angle was significantly greater in BCLP patients than the control group.
This result is in agreement with result of Shetye study [12] and is an approvement for the facial vertical growth tendency in BCLP patients.
2) Sagittal dimension
• SNB and S.N.Pog angles didn’t show significant difference between BCLP and control groups. And this result is in agreement with Silva Filho and Capelozza studies [2,9].
In contrary to our findings, Jahanbin study showed significant differences in SNB and S.N.Pog parameters between BCLP and control groups. This controversy could be because of different type of radiographs evaluated in our studies (lateral cephalograms versus cone beam computed tomography). And also Shetye reported a significant difference in SNB between the unilateral cleft lip and palate patients and non-cleft subjects [12]. The controversy could be related to our different cleft subtypes we’ve studied.
• Facial angle was significantly decreased in BCLP patients than the control group.
• Pog-N.perp was significantly increased in BCLP patients than the control group.
These two parameter changes show the retrusion of chin in BCLP patients. Shetye also reported a significant difference in facial angle between unilateral cleft lip and palate patients and non-cleft subjects. He studied unoperated non-syndromic unilateral cleft lip and palate patients; his ample was 30 adult indian patients over 18 years old. He also reported no significant difference in Pog-N.perp between the unilateral cleft lip and palate and non-cleft subjects [12].
Shrestha A et al. examine the relationship between mandibular volume and craniofacial morphology in patients with cleft lip and palate using Cone Beam Computed Tomography (CBCT) and to Compare These Findings with Control (noncleft) patients during the deciduous dentition period. The results showed that no statistically significant differences in mandibular volume among the groups [13].
Fowler PV et al. studied to establish baseline lateral craniofacial morphology and soft tissue profile outcomes for New Zealand children with complete unilateral and Complete Bilateral Cleft Lip and Palate (CUCLP/CBCLP) and determine differences in relation to demographic characteristics including cleft type, sex and ethnicity. The results showed that CUCLP had greater midface and mandibular retrusion than CBCLP. Females had greater midface and mandibular prominence and smaller nasal projections. The Pacific and Māori groups had more retrusive midfacial profiles, and the Pacific group had more prominent mandibles [14].
Aiyesha Wahaj et al. studied to compare mandibular vertical asymmetry between cleft lip palate and normal class I occlusion subjects. The results showed that statistically significant differences in both condylar and ramal asymmetry index but over all intergroup comparison of condylar plus ramal height asymmetry index did not show any significant result. Mandible in cleft lip and palate subjects was found to be normal. However, in unilateral cleft lip and palate a difference was found in condyle, ramal and gonial angle between cleft and non-cleft side [15].
Conclusion
According to our findings, unoperated non-syndromic BCLP patients are characterized by following features: Tendency to vertical growth of face, an obtuse Gonial angle, a smaller ramus length, a greater mandibular plane angle and retrusion of chin. Mandibular morphologic characteristics of BCLP patients could be considered as an intrinsic part of this malformation and not just as a consequence of the surgical or other treatments.
References
- Jahanbin A, Eslami N, Hoseinizarch H, Kobravi S. Comparative evaluation of cranial base and facial morphology of cleft lip and palate patients with normal individuals in cone beam computed tomography. J Craniofac Surg. 2015; 26: 785-788.
- Capelozza Júnior L, Taniguchi SM, da Silva Júnior OG. Craniofacial morphology of adult unoperated complete unilateral cleft lip and palate patients. Cleft Palate Craniofac J. 1993; 30: 376-381.
- Kaduk WM, Grabowski R, Gundluch KK. Position of the hyoid bone in cleft lip, alveolus, and palate: variation of normal anatomy or sign accompanying the malformation? Cleft palate craniofac J. 2003; 40: 1-5.
- Shetye PR1, Evans CA. Midfacial morphology in adult unoperated complete unilateral cleft lip and palate patients. Angle Orthod. 2006; 76: 810-816.
- Buyuk SK, Celikoglu M, Benkli YA, Sekerci AE. Evaluation of the Transverse Craniofacial Morphology of Adolescents with Repaired Unilateral Cleft Lip and Palate Using Cone-Beam Computed Tomography. J Craniofac Surg. 2016; 27: 1870-1874.
- Mozafar Khazaei, Somaieh Ghanbari, Mansour Rezaei, Ali Asghar Alipour, Saber Khazaei, et al. Evaluation of cleft lip and palate frequency and related risk factors in infants born in Kermanshah hospitals (2001-2008). Journal of Isfahan Dental School. 2010; 6: 298-304.
- Celikoglu M, Halicioglu K, Buyuk SK, Sekerci AE, Ucar FI, et al. Condylar and ramal vertical asymmetry in adolescent patients with cleft lip and palate evaluated with cone-beam computed tomography. Am J Orthod Dentofacial Orthop. 2013; 144: 691-697.
- Hayashi I, Sakuda M, Takimoto K, Miazaki T. Craniofacial growth in complete unilateral cleft lip and palate: A roentgeno-cephalometric study. Cleft palate J. 1976; 13: 215-237.
- Da Silva Filho OG, Carvalho Lauris RC, Capelozza Filho L, Semb G, et al. Craniofacial morphology in adult patients with unoperated complete bilateral cleft lip and palate. Cleft Palate Craniofac J. 1998; 35: 111-119.
- Kurt G, Bayram M, Uysal T, Ozer M. Mandibular asymmetry in cleft lip and palate patients. Eur J Orthod. 2010; 32:19-23.
- Abuhijleh E, Aydemir H, Toygar-Memikoğlu U. Three-dimensional craniofacial morphology in unilateral cleft lip and palate. J Oral Sci. 2014; 56: 165-172.
- Shetye PR1, Evans CA. Midfacial morphology in adult unoperated complete unilateral cleft lip and palate patients. Angle Orthod. 2006; 76: 810-816.
- Abhishekhi Shrestha, Masahiro Takahashi, Tetsutaro Yamaguchi, Mohamed Adel, Mayu Furuhata, Three-dimensional evaluation of mandibular volume in patients with cleft lip and palate during the deciduous dentition period. Angle Orthodontis. 2019. [Epub ahead of print].
- Fowler PV, Wholley C, Perry JG, Thompson JMD. Craniofacial morphology and soft tissue profile outcomes for complete unilateral and complete bilateral cleft lip and palate in New Zealand. Orthod Craniofac Res. 2019; 22: 139-146.
- Wahaj A, Ahmed I, Erum G. Comparison of Mandibular Asymmetry between Cleft Lip Palate and Normal Subjects. J Pak Dent Assoc. 2014; 23: 70-75.