SciBase Journals
SciBase Dentistry and Oral Sciences
ISSN 2996-363X
- Article Type: Short Commentary
- Volume 1, Issue 1
- Received: Oct 28, 2023
- Accepted: Sep 07, 2023
- Published Online: Sep 14, 2023
Evaluation of Bolton’s Class II Patients Treated with EXT Premolars with Appropriate Finishes in Orthodontic Treatment
Siamak Hematpour1; Gholamreza Heidari2*; Mohammad Sadegh Nazari3; Leila Bazvand4
1Assistant Professor, Department of Prosthodontic, Dental Branch, Islamic Azad University, Tehran, Iran.
2Assistant Professor of Dentistry, Department of Orthodontics, School of Dentistry, Lorestan University of Medical Science.
3Post Graduated student, Department of Orthodontics, School of Dentistry, Mashhad University of Medical Science, Mashhad. Iran.
4Endodontics Specialist, Department of Endodontics, School of Dentistry, Lorestan University of Medical Science.
*Corresponding Author: Gholamreza Haidari
Department of Orthodontics, School of dentistry, Lorestan University of Medical Science, Khorramabad, Iran.
Tel: +989123241098;
Email: Ghrh61@yahoo.com
Abstract
Background and aim: One of the requirements for orthodontic treatment is, making appropriate final occlusion and Finishing correctly. More frequently in Class II patients with maxillary pre molar extraction, to make the final occlusion is impossible, This is due to the disruption of Bolton rate by Extraction maxillary premolars, because the mean mesiodistal width of the premolar tooth is greater than the migration rate of the maxillary first molar tooth from the buccal groove mandibular first molar to the embrasure between the fifth and sixth teeth. For these reasons, to make an appropriate final occlusion, more frequently we need the TIPR (total inter proximal reduction) in mandible. in this study, we examined patients with Class II who were treated with extraction of maxillary first pre molars and its treatment with selective TIPR reached to the appropriate final occlusion, to we’ve got the ultimate good of Bolton is calculated.
Materials and methods: This study is a semi-experimental. 44 casts were evaluated before and after treatment for Class II patients. Casts by scanning (3D) scan basis by Software Maestro 3D ortho studio within MOD teeth 6 to 6 Top down pointed and measured in 3D, and the anterior and overall ratio for each sample were calculated. These measurements were performed with a precision digital caliper 0/01 too. The amount of stripping, were obtained from difference between the total mesiodistal width of mandibular 6 to 6 before and after treatment. Data were analyzed by the software PASW Statistics Data Editor.
Results: Overall Bolton’s ratio, respectively, 101/62 ± 0/9SD in men and 101/70± 0/92 SD in women and anterior Bolton’s ratio 74/21 ± 2/13 SD men and 74/42 ± 1/75 SD were women. The amount of stripping was done 3/26 ± 1/25 SD in men and 3/22 ± 1/11 SD in women. Bolton anterior and overall ratios in both sexes, the difference was not statistically significant (ant.p = 0/852 overall. p = 0/346). With respect to the correlation, there is a significant relationship between the anterior and overall Bolton of men and stripping and also between the anterior primary Bolton of women and stripping (c = 0/571). Between overall Ratio and anterior Ratio before and after treatment are correlated. Comparison between the two methods of measurement, no significant differences were observed.
Conclusions: In treated Class II patients with maxillary pre molar extraction, to obtain a proper finishing, we should obtain a proper Bolton’s ratio for these patients with selective stripping witch is showed in this study and most of the time it’s impossible to reach an appropriate final occlusion without striping from the lower arch. Measured using 3D, the clinically accurate method than manually caliper 0/01mm is more accurate but does not show a statistically significant difference.
Keywords: Bolton ratio; Anterior ratio; Overall ratio; Stripping; Malocclusion CL II.
Citation: Hematpour S, Heidari G, Nazari MS, Bazvand L, et al. Evaluation of Bolton’s Class II Patients Treated with EXT Premolars with Appropriate Finishes in Orthodontic Treatment. SciBase Dent Oral Sci. 2023; 1(1): 1004.
Introduction
One of the requirements of orthodontic treatment is the establishment of a proper final occlusion and proper Finishing, because otherwise the treatment will relapse [1, 2]. In most cases, in class II patients with bilateral upper premolar extraction, it is impossible to schedule a suitable final occlusion for three reasons: 1- Increased IMPA in most patients in class II [3], 2- Reduction of high inclination during retraction of the anterior teeth of the upper jaw, even with the use of more torque brackets [4], 3. Lack of proper bolton ratio in most patients (In most people, the mesiodistal width of the mandibular teeth than of the maxilla higher than of normal) [5].
In 1958, Bolton first conducted a study on dental size inconsistency and its relationship to analysis and treatment of malocclusion. His aim in this study was to analyze a group with ideal occlusion and to determine whether there was a mathematical relationship between the total length of the maxillary with mandibular arches or also parts of the maxillary arches with the mandible? He concluded that for optimal occlusion between the maxillary and mandibular teeth, the ratio of the total mesiodistal width of the first molar teeth on one side to the first molar on the opposite side of the mandible to the maxilla (Overall ratio) should be about 91.3% and the total ratio The mesiodistal width of the anterior 6 mandibular to maxillary (Anterior ratio) is about 77.2% [6]. Extraction in any of the compounds (extraction of premolars) leads to a decrease in the overall Bolton ratio. However, Dental size discrepancy with extraction of all first premolars is the highest. While discrepancy with extraction of all second premolars is the least. Also, based on the combination of teeth selected for extraction, the difference in the overall Bolton ratio between men and women is significant [7]. Other researchers have conducted extensive research on the Bolton index and the severity of tooth size discrepancies in different malocclusions among different communities and races and obtained different results [5, 8-12].
For the above reasons, in the final stages of these patients, Establishing overjet and overbite and posterior occlusion and of course establishing and creating functional occlusion and proper support in most cases without stripping the mandibular teeth, even by changing the tip of the lower canine teeth in the direction It is impossible to reduce the mesiodistal width and increase it in the maxilla to add to the mesiodistal width maxilla. Factors affecting the amount of reduction, the amount of primary bolton in the patient and the amount of IMPA changes during treatment, etc.Research has been conducted on the proportion of bolton in different groups of malocclusion as well as in different races, but no research has been done on the optimal bolton ratio in Class II patients treated with upper premolar EXT with appropriate occlusion. (9 and 13), Therefore, in this study, we decided to review the patients of class II who referred to the private clinic in Tehran in 2010-12, who were treated with upper premolars EXT, and in their treatment with selected TIPR, we have reached a suitable final occlusion, Calculate the appropriate bolton.
Materials and methods
The study was semi-experimental. First, all the files in the orthodontics department of the School of Dentistry of the Islamic Azad University of Tehran were examined and selected qualified samples were selected from them. The inclusion criteria for the study were as follows: The study casts all belonged to Class II patients treated with upper bilateral EXT premolar and all the casts were healthy, the samples had a full class II molar relationship and a Class I canine relationship, Samples with normal overbite 2-3 mm, and normal overjet were 2-3 mm [14], There was no space between the teeth, The teeth were completely alignment, Occlusion in all casts was ideal and proper, of course, functional and supportive occlusion was established (On clinical examination in patients’ calls).
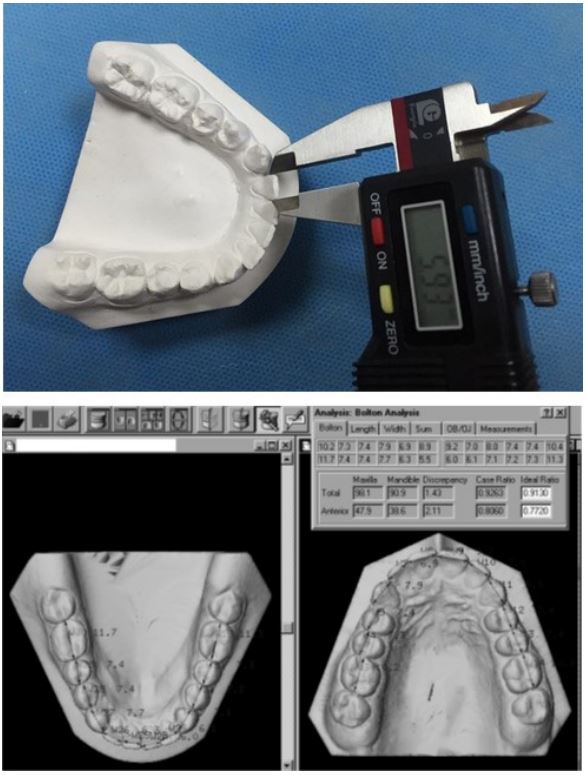
Casts that did not meet the above conditions were removed from the sample. The number of samples according to the results of the pilot study (according to the type of study, was performed on 10 male and 10 female pilot samples and considering the average standard deviation of the main variable Bolton discrepancy 2.8 and the minimum difference Significantly equal to 2 units, sample size was estimated using the comparison option of two averages for determining the sample size of Minitab software, considering α = 0.05 and β = 0.2, 22 people in each sex) estimated and their casts They were examined before and after treatment. The casts were scanned by a 3D scanner and by Maestro 3D ortho studio studio (Figure 1), the mesodistal width of the teeth 6 to 6 upper and 6 to 6 lower was punctuated and measured in 3 dimensions and pre-treatment & post-treatment overall ratio and pre-treatment & post-treatment anterior ratio for each sample were calculated. These measurements were also performed by digital caliper with an accuracy of 0.01. To reduce errors and prevent bias, all casts were measured twice (several days apart) by one person and the numbers obtained were then calculated by calculating the total mesiodistal width of the teeth. This was done twice to ensure the total of these measurements. The figures obtained are in the Bolton formula and pre-treatment & post-treatment overall ratio and pre-treatment & post-treatment anterior ratio for each sample, respectively, Calculated. The amount of stripping was obtained from the difference between the total mesodistal width of 6 to 6 mandibles before and after treatment. The data were analyzed by PASW Statistics Data Editor Software.
Results
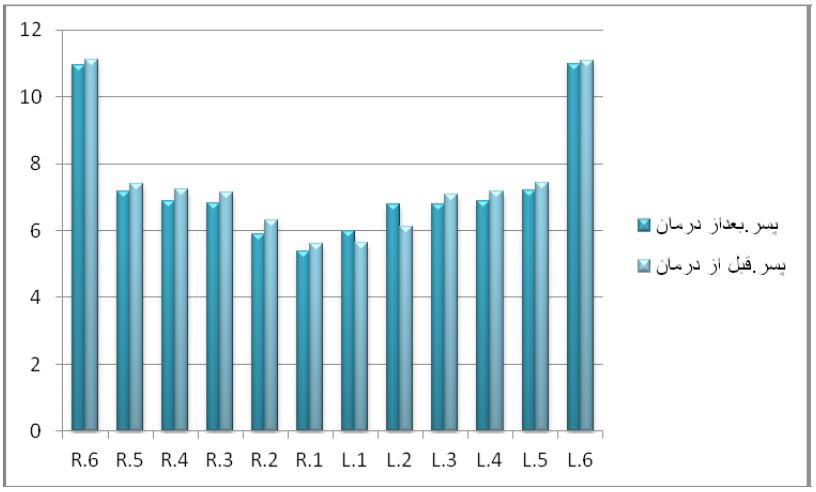
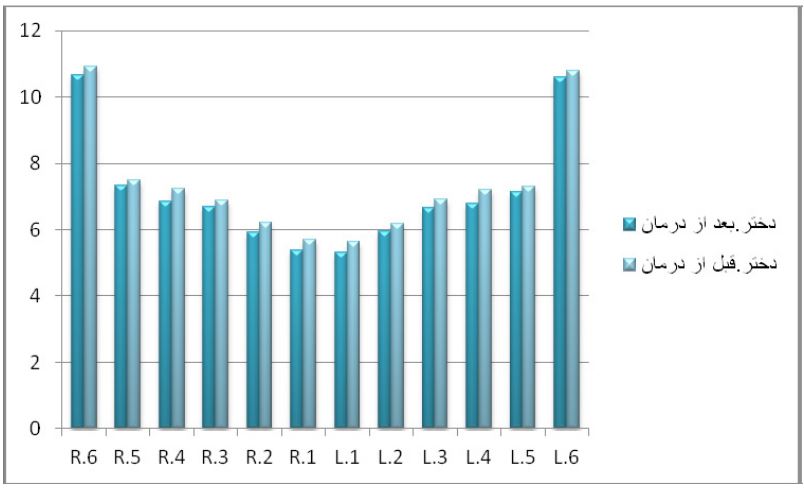
The study was performed on 44 casts according to the type of study. The subjects were 50% girls and 50% boys, with a mean age of 21 years with a minimum age of 14 years and a maximum of 30 years. All samples were Class II patients with bilateral maxillary premolar extraction and suitable final finishing. The mesiodistal width of the maxillary and mandibular teeth was measured before and after treatment of patients with two digital caliper methods with an accuracy of 0.01 mm and maestro 3D ortho studio software. The mean mesiodistal width of 6-6 upper and lower before and after treatment is presented in both measurement methods in Tables 1 to 4.
Table 1: Distribution of the studied people according to the mesiodistal width of the maxillary teeth after orthodontic treatment disaggregated by gender, measured with Maestro 3D ortho studio software.
| 6 | 5 | 3 | 2 | 1 | 1 | 2 | 3 | 5 | 6 | |
|---|---|---|---|---|---|---|---|---|---|---|
| female | 10.56±0.52 | 7.16±0.52 | 7.88±0.28 | 7.41±0.38 | 8.9±0.39 | 8.83±0.48 | 7.25±0.35 | 7.88±0.37 | 7.28±0.39 | 10.55±0.54 |
| male | 10.6±0.56 | 7.34±0.59 | 8.12±0.55 | 7.12±0.32 | 9.12±0.66 | 9.3±0.52 | 7.17±0.53 | 8.28±0.47 | 7.3±0.4 | 10.81±0.52 |
Table 2: Distribution of the studied subjects according to the mesiodistal width of the mandibular teeth before and after orthodontic treatment disaggregated by gender, measured with Maestro 3D ortho studio studio software.
| 6 | 5 | 4 | 3 | 2 | 1 | 1 | 2 | 3 | 4 | 5 | 6 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| before | female | 10.56 ± 0.52 | 7.5±0.32 | 7.22±0.36 | 6.89±0.26 | 6.21±0.31 | 5.7±0.36 | 5.64±0.36 | 6.19±0.29 | 6.9±0.37 | 7.21±0.54 | 7.31±0.31 | 10.78±0.5 |
| male | 10.6 ± 0.56 | 7.39±0.4 | 7.22±0.46 | 7.12±0.49 | 6.29±0.34 | 5.6±0.35 | 5.63±0.21 | 6.1±0.41 | 8.28±0.47 | 7.19±0.3 | 7.43±0.28 | 11.81±0.4 | |
| after | female | 10.67±0.54 | 7.16±0.40 | 6.85±0.33 | 6.68±0.23 | 5.91±0.26 | 5.36±0.32 | 5.31±0.29 | 5.94±0.34 | 6.64±0.40 | 6.79±0.36 | 7.15±0.35 | 10.59±0.55 |
| male | 10.95±0.52 | 7.34±0.44 | 6.87±0.31 | 6.81±0.41 | 5.88±0.38 | 5.36±0.36 | 5.36±0.30 | 5.98±0.43 | 6.78±0.45 | 6.87±0.40 | 7.20±0.41 | 10.97±0.45 |
Table 3: Distribution of the studied subjects according to the mesiodistal width of the maxillary teeth after orthodontic treatment dis- aggregated by gender, measured by digital caliper.
| 6 | 5 | 4 | 3 | 2 | 1 | 1 | 2 | 3 | 4 | 5 | 6 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| female | 10.63±0.36 | 7.33±0.37 | 7.78±0.31 | 7.27±0.35 | 8.98±0.33 | 8.96±0.39 | 7.17±0.32 | 7.78±0.36 | 7.31±0.32 | 10.46±0.36 | 7.4±0.36 | 10.90±0.54 |
| male | 10.75±0.49 | 7.34±0.52 | 8.10±0.48 | 7.07±0.49 | 9.04±0.62 | 9±0.53 | 7.9±0.42 | 8.3±0.47 | 7.38±0.45 | 10.74±0.47 | 7.43±0.29 | 11.16±0.43 |
Table 4: Distribution of the studied subjects according to the mesiodistal width of the mandibular teeth before and after orthodontic treatment disaggregated by gender, measured by digital caliper.
| 6 | 5 | 4 | 3 | 2 | 1 | 1 | 2 | 3 | 4 | 5 | 6 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| before | female | 10.88±0.56 | 7.52±0.29 | 7.14±0.46 | 7.07±0.37 | 6.14±0.41 | 5.80±0.35 | 5.80±0.35 | 6.17±0.41 | 6.99±0.46 | 7.12±0.30 | 7.4±0.36 | 10.90±0.54 |
| male | 10.22±0.48 | 7.36±0.44 | 7.15±0.31 | 7.18±0.45 | 6.20±0.35 | 6.67±0.32 | 5.62±0.32 | 6.22±0.37 | 7.12±0.37 | 7.2±0.28 | 7.43±0.29 | 11.16±0.43 | |
| after | female | 10.73±0.50 | 7.34±0.30 | 6.85±0.38 | 6.65±0.31 | 5.85±0.28 | 5.37±0.30 | 5.29±0.32 | 5.91±0.36 | 6.67±0.41 | 6.84±0.36 | 7.25±0.37 | 10.72±0.5 |
| male | 10.04±0.48 | 7.14±0.49 | 6.74±0.33 | 6.67±0.43 | 5.81±0.28 | 5.42±0.30 | 5.42±0.28 | 5.88±0.32 | 6.66±0.39 | 6.76±0.37 | 7.17±0.40 | 11.03±0.4 |
There was no significant difference between the two measurement methods (digital caliper with an accuracy of 0.01 mm and maestro 3D ortho studio software). The obtained figures were placed in the Bolton formula and the overall Ratio and anterior ratios before and after treatment were calculated for each sample, respectively. The mean overall Ratio and anterior Ratio before and after treatment are presented in Table 5 to 8.
Table 5: Distribution of the studied subjects according to Bolton index before treatment, taking into account the mesiodistal width of the upper first premolar disaggregated by gender, mea- sured with Maestro 3D ortho studio software.
| Anterior ratio | Overall ratio | |||||
|---|---|---|---|---|---|---|
| Min | Mean±Std | Max | Min | Mean±Std | Max | |
| Female | 76.84% | 79.45 ± 3.04% | 88.60% | 90.03% | 91.45 ± 1.67% | 96.49% |
| Male | 71.64% | 78.33 ± 2.85% | 83.34% | 90.08% | 91.46 ± 1.03% | 94 % |
Table 6: Distribution of studied subjects according to Bolton index before treatment without taking into account the mesiodistal width of the upper first premolar disaggregated by gender, measured with Maestro 3D ortho studio software.
| Anterior ratio | Overall ratio | |||||
|---|---|---|---|---|---|---|
| Min | Mean±Std | Max | Min | Mean±Std | Max | |
| female | 76.84% | 79.45 ± 3.04% | 88.60% | 101.85% | 105.32 ± 1.98% | 108.65% |
| male | 71.64% | 78.33 ± 2.85% | 83.34% | 102.66% | 105.34 ± 1.39% | 108.35 % |
Table 7: Distribution of study subjects according to Bolton index after treatment disaggregated by gender, measured with Maestro 3D ortho studio software.
| Anterior ratio | Overall ratio | |||||
|---|---|---|---|---|---|---|
| Min | Mean±Std | Max | Min | Mean±Std | Max | |
| female | 71.46% | 74.42 ± 1.75% | 78.27% | 100.16% | 101.70 ± 0.92% | 103.39% |
| male | 71.15% | 74.21 ± 2.13% | 77.84% | 100.07% | 101.62 ± 0.90% | 102.73% |
Table 8:Distribution of studied subjects according to Bolton index before and after treatment disag- gregated by gender, measured by digital caliper.
| Anterior ratio | Overall ratio | ||||||
|---|---|---|---|---|---|---|---|
| Min | Mean±Std | Max | Min | Mean±Std | Max | ||
| before | female | 75.30% | 79.11 ± 2.67% | 83.13% | 88.11% | 90.79 ± 1.78% | 93.64% |
| male | 75.36% | 79.07 ± 2.42% | 84.20% | 88.81% | 90.89 ± 1.48% | 94.36% | |
| after | female | 71.07% | 74.25 ± 2.36% | 79.10% | 99.61% | 101.90 ± 1.20% | 104.02% |
| male | 71.78% | 74.39 ± 1.76% | 77.16% | 100.20% | 101.50 ± 1.03% | 103.60% | |
Table 9: Distribution of studied people according to the de- gree of stripping of the mandibular teeth disaggregated by gender by two measurement methods.
| measurement | Min | Mean±Std | Max | |
|---|---|---|---|---|
| Maestro 3D ortho studio | female | 1.25 mm | 3.22 ± 1.11 mm | 5.13 mm |
| male | 0.98 mm | 3.26 ± 1.25 mm | 5.67 mm | |
| لاتیجیدسیلوک | female | 1.31 mm | 3.37 ± 1.21 mm | 5.32 mm |
| male | 2.15 mm | 3.50 ± 1.02 mm | 6.03 mm |
According to the T-test statistical test, there was no significant statistical difference between the anterior and overall ratio boltons in both sexes (ant. ratio p=0/852, overall. ratio p=0/346, strip p=0/747). There was correlation between overall Ratio and anterior Ratio after treatment and overall Ratio and anterior Ratio before treatment, which is statistically significant and determines when the anterior. Ratio increase, overall. Ratio also increases proportionally.
From the difference between 6 and 6 lower mesodistal width before and after treatment, the stripping rate was calculated and presented in Table 9.
According to the correlation coefficient, there was a significant relationship between the initial anterior bolton ratio of girls and the rate of stripping (c = 0.571). This means that the higher the initial bolton rate, the greater the amount of stripping required. There was also a significant relationship between anterior and overall ratio primary bolton in boys and the rate of stripping (ant. ratio C=0.587, overall. ratio C=0.648).
Discussion
In most cases, in Class II patients with bilateral upper premolars extraction, it is impossible to establish a suitable final occlusion [5], therefore, in the final stages of these patients, establish proper overjet and overbite and posterior occlusion in most cases without dental stripping Lower jaws are impossible. Therefore, in order to create a suitable final occlusion, most of the Total Inter Proximal Reduction (TIPR) in the mandible is required. Factors affecting the rate of reduction include the amount of primary bolton in the patient, the rate of increase in IMPA during alignment, and the rate of decrease in U1 during retraction of upper incisors. The findings of this study, which examined the ratio of Cl II patients’ boltons with upper premolar extraction with suitable finishing, showed that to treat these patients, it is necessary to obtain a suitable bolton by selective stripping of the mandible and it is not possible to treat such patients by relying on Bolton’s standard ratio. Since the most important goal of orthodontic treatment is to achieve the best functional condition, stability of treatment and proper supportive occlusion along with beauty, to achieve this goal, at the end of treatment, proper final occlusion and proper finishing should be created because Otherwise, treatment will be relapsed due to lack of overjet and overbite final or the establishment of a molar relationship beyond class II (1 and 2). When there is a mismatch in the size of the teeth, it will not be possible to obtain normal overbite and overjet, and normal overbite and overjet are also prerequisites for treatment stability and supportive occlusion. The maximum stripping rate that can be done is 4-6 mm [15]. In the studied cases, the mean was 3.24±0.02.
In the present study, like the studies conducted in 2004 by Edward and Villanueva-bemabe, in 2006 by Dr. Hamid Reza Fattahi et al. And in 2010 by Sanjay naduwinmani et al., A statistically significant difference between the anterior and overall bolton ratio in two There was no gender between men and women (5 and 8). However, in studies such as the Laveh study in 1972, the research of the University of Michigan Development Center in 1979, the study of chowsha-szule and her colleagues in 2010, and the research of insigammuqbil in 2011 that Examining the ratio of Bolton in different races and groups of different malocclusions, there was a statistically significant difference between the anterior and overall bolton ratios in both sexes [9, 12, 16, 17].
In this study, a comparison was made between the two methods of measuring the mesodial width of teeth. The first method was to use a digital caliber with an accuracy of 0.01 mm and the second method was to use maestro 3D ortho studio software, which did not have a significant statistical difference between the two methods to obtain the Bolton ratio. Like a study conducted in 2001 by James et al. comparing the measurement of Bolton analysis with computer methods and common methods [18]. Hend mohammed EL-zanaty et al. (2010) also conducted a study in 3D called dental model replacement for gypsum models, which resulted in a similar result to the present study [19]. In 2016, Shaji T. Varghese et al. conducted a study to evaluate the effect of premolar extraction on overall ratio and tooth size discrepancies.They concluded that in formulating treatment plans, including premolar extraction, significant tooth size discrepancy could change reciprocally after extraction [7].
In 2019, Jabri MA et al. conducted a review article to compare tooth size discrepancy among class I, II, and III malocclusions. The results of their study showed that many researchers did not show a statistically significant difference, but the data, especially the data related to the subclasses of the Angle malocclusion classification, are not sufficient among these studies. Therefore, further studies are needed to interpret this correlation [20].
There have been many studies examining the Bolton index in different races [5, 8-12], but so far there has been a study on the Bolton ratio of CL II patients treated with upper bilateral premolar extraction and total lower jaw stripping and final finishing appropriate have arrived, not done.
In the studied cases, the ratio of overall and anterior boltons of patients without taking into account one of the upper molar teeth on the left and right, is 105.34±1.39 in men and 105.32±1.98 in women and it was 78.33±2.85 in men and 79.45±3.04 in women, respectively. After treatment, taking into account the effect of stripping and reducing the mesiodistal width of the mandibular teeth in men, about 3.26±1.25 and 3.22±1.11 in women, the overall and anterior bolton ratio was 101.62±0.9, respectively in males and 101.7±0.92 in females and 74.22±1.13 in males and 74.42±1.75 in females decreased. These numbers show that standard boltons cannot be used to achieve a suitable finishing in these patients (the overall standard bolton is 91.3% and the ratio of the anterior standard bolton is 77.2%) and requires a new bolton rate definition for these patients.
Conclusion
In this study, it was found that the treatment of CL II patients with upper premolar extraction with appropriate finishing requires a new bolton ratio (overall and anterior bolton ratio of 105.3 and 78.8, respectively) and cannot be considered according to bolton standard achieved an ideal finishing and proper functional and supportive occlusion. Also, the use of the 3 D measurement method is clinically more accurate than the manual caliper method with an accuracy of 0.01 mm, but it is not statistically significant. The 3D method requires more time to measure due to the need to reconstruct and review in three dimensions.
References
- Okamoto M, Takada K, Yasuda Y, Bishara S. relapse after orthodontic treatment and its correlation with dentoskeletal morphology. Clin Orthod Res. 2000; 3: 173-181.
- Burlingame, Michelle L, MS. The effects of an Anterior Bolton Discrepancy on the long term stability of lower incisors. State University of New York at Buffalo. 2010; 85: AAT 1477151.
- MR Freitas, DV Lima, KMS Freitas, G Janson, JFC Henriques, et al. Cephalometric evaluation of Class II malocclusion treatment with cervical headgear and mandibular fixed appliances. European Journal of Orthodontics. 2008; 30: 477-482.
- EAO’ H I G G I N S. The Influence of Maxillary Incisor Inclination on Arch Length. British Journal of Orthodontics. 1999; 26: 97-102.
- Fattahi H R, Pakshir H R, Hedayati. Comparison of tooth size discrepancies among different malocclusion groups. European Journal of Orthodontics. 2006; 28: 491-495.
- Bolton Wayne A. Disharmony in tooth size and its relation to the analysis and treatment of malocclusion. The Angle Orthod. 1958; 28: 113-130.
- Varghese ST, Yerasi PR, Jose LK, Mohammed Haris TP, Mathew T, Ealla KK, et al. Outcome of premolar extractions on Bolton’s overall ratio and tooth size discrepancies in South India. J Int Soc Prevent Communit Dent. 2016; 6: 309-315.
- Naduwinmani, Sanjay Laxman; Jyosna, Preetham Naduwinmani; Krishna US. Nayak. Evaluation of Bolton’s Tooth Width Ratios in Crowded and Non-Crowded Dentitions in Class I and Class II skeletal bases among the South Indian population: An In-vitro Study. International Journal of Contemporary Dentistry. 2010. 1: 99-106.
- Barbara We dry chowska-Szulc. Overall and anterior Bolton ratio in Class I, II, and III orthodontic patients. European Journal of Orthodontics. 2010; 32: 313-318.
- Susan NAl-Khateeb, Elham SJ Abu Alhaija. Tooth Size Discrepancies and Arch Parameters among Different Malocclusions in a Jordanian Sample. Angle Orthod. 2006; 76: 459-465.
- Mojgan Kachoei, Mohammad-Hosein Ahangar-Atashi. Bolton’s intermaxillary tooth size ratios among Iranian schoolchildren. Med Oral Patol Oral Cir Bucal. 2011; 16: e568-572.
- InsigamMuqbil. Analysis of Bolton’s tooth size discrepancy for a referred UK population. University of Birmingham Research Archive. 2011.
- Aravjo E, Souki M. Bolton anterior tooth size discrepancies among different malocclusion groups. Angle Orthod. 2003; 73: 307-313.
- Proffit WR and Fields HW. Contemporary Orthodontics. Chicago: Mosby Year Book. 2019; 1-15.
- Bolton Wayne A. Disharmony in tooth size and its relation to the analysis and treatment of malocclusion. The Angle Orthod. 1958; 28: 113-130.
- Chang JZ, Chen YJ, Chang FH, Yao JC, Liu PH, Chang CH, et al. Morphometric analysis of mandibular growth in skeletal Class III malocclusion. J Formos Med Assoc. 2006; 105: 318-328.
- Behdin, Verhram. Examining the prevalence of dental and maxillofacial abnormalities among Zoroastrian students aged 8-10 and 12-14 years old in Tehran in the academic year 1379-80, Thesis No. 1752, School of Dentistry, Islamic Azad University. 1380.
- James J. Tomassetti, Louis J. Taloumis, John M, et al. A Comparison of 3 Computerized Bolton Tooth-Size Analyses with a Commonly Used Method. Angle Orthod. 2001; 71: 351-357.
- Hend Mohammed El-Zanaty, Amr RagabEl-Beialy, Amr MohammedAbou El-Ezz, Khaled HazemAttia, Ahmed RagabEl-Bialy, et al. Three-dimensional dental measurements: An alternative to plaster models. American Journal of Orthodontics and Dentofacial Orthopedics. 2010; 137: 259-265.
- Jabri MA, Wu S, Zhang Y, Ma J, Wang L, et al. A Review on Comparison of Tooth Size Discrepancies among Angle’s Class I, II, and III Malocclusion: Is There a Significance? J Contemp Dent Pract. 2019; 20: 994-999.