SciBase Journals
SciBase Dentistry and Oral Sciences
ISSN 2996-363X
- Article Type: Research Article
- Volume 1, Issue 2
- Received: Nov 09, 2023
- Accepted: Dec 20, 2023
- Published Online: Dec 27, 2023
Blue-Violet Light-Blocking Eye Protectors in Dental Practice: A Preliminary Study
Eiji Mitate1,2*; Shigeki Moriwaki3; Ichiro Masui2
1Department of Oral & Maxillofacial Surgery, Faculty of Medicine, Kanazawa Medical University, 1-1, Daigaku, Uchinada, Kahoku, Ishikawa 920-0293, Japan.
2Oral and Maxillofacial Surgery, Hirose Hospital, 1-21-11, Watanabe-Dori, Chou-ku, Fukuoka-City, Fukuoka 810-0004, Japan.
3Isuzu Glass Ltd, 1-53, Rinku Ohrai-kita, Izumisano-City, Osaka 598-0048, Japan.
*Corresponding Author: Eiji Mitate
Department of Oral & Maxillofacial Surgery, Faculty of Medicine, Kanazawa Medical University 1-1 Daigaku, Uchinada, Kahoku, Ishikawa 920-0293, Japan.
Email: mitateeiji@gmail.com
Abstract
Healthcare professionals are exposed to various intense light sources during dental practice. Of particular concern is blueviolet light (wavelength 380-500 nm), which can impact retinal health, necessitating effective mitigation strategies. In this study, we assessed the practical utility of lenses designed to reduce blue-violet light to wavelengths of approximately 420 nm or shorter within the dental practice setting. Two dentists and four dental hygienists participated in the study. The participants wore either blue-light-reducing lenses or lenses with no effect for one month. The degree of eye strain was evaluated using flicker values. The results revealed that four of the six participants experienced reduced eye strain while wearing blue-violet light-reducing lenses. In conclusion, this study addresses the acknowledged impact of blue-violet light on retinal health. However, the long-term prognosis remains uncertain. Therefore, considering the potential unknown effects, it is necessary to discuss the use of blue-violet light-cut lenses in everyday practice as a risk-management strategy.
Keywords: Dental practice; Eye strain; blue-violet light; Blue light cut; Flicker value.
Abbreviations: LED: Light emitting diode.
Citation: Mitate E, Moriwaki S, Masui I. Blue-Violet Light-Blocking Eye Protectors in Dental Practice: A Preliminary Study. SciBase Dent Oral Sci. 2023; 1(2): 1007.
Introduction
Dental professionals frequently encounter a range of intense light sources in their work environment, including the lighting in examination rooms, dental chair units, contrast-free lights in operating theatres, photopolymerization resin irradiators, and office whitening irradiators. These working conditions often lead to eye strain. While the adverse effects of blue-violet light (wavelength: 380-500 nm) on the retina have been documented, and blue-violet light-cut glasses are available for computer users, the incorporation of this blue-violet light-cut feature in eye protectors for dental professionals remains limited. Given the demanding nature of their work environments and the strain it places on their eyes, the introduction of blue-light-cut functionality was deemed necessary.
The ultraviolet absorbing filter ITY430 (Isuzu Glass Ltd., Osaka, Japan) can reduce light to wavelengths of approximately 420 nm and below (Figure 1). This study aims to assess the effectiveness of ITY430 in reducing eye strain by eliminating blue-violet light and developing an eye protector that selectively allows only light that is gentle on the eyes to pass through.
Subjects and methods
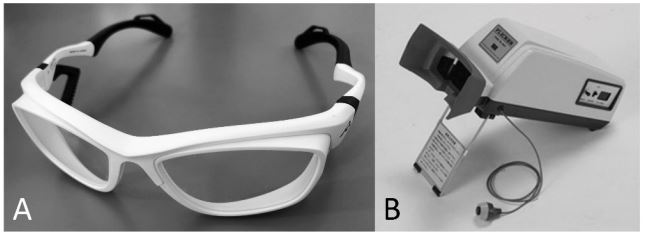
Subjects in this study were two dentists (A,B) and four dental hygienists who wore eye protectors (Figure 2A) with ITY430 treated lenses (ITY group) and eye protectors without any light reduction treatment (N group) for a duration of one month. Flicker values were measured to determine eye strain using a Flicker Value Measuring Instrument Type II (Figure 2B, Takei Kiki Kogyo, Niigata, Japan). Flicker values were compared before and after wearing the eye protector. If the flicker value remained the same or increased, it indicated an improvement (reduction) in eye strain, whereas a decrease in the flicker value indicated a worsening of eye strain. Pearson’s chi-square test was used for statistical processing, with p<0.05 indicating a significant difference.
Method of measuring eye strain: Eye strain was quantified by measuring the flicker value using a Flicker Value Measuring Instrument Type II. The flicker value corresponds to the threshold at which light begins to appear to flicker (flicker fusion frequency) when exposed to high frequency flashing light (flicker light). The measurement method was based on a fixed distance of approximately 50 cm between the test eye and the light source. The light source was presented through a circular window with a viewing angle of 0.4°, and the flicker frequency was adjusted accordingly. The illuminance in the flicker field of view was maintained at 500 lx ± 10%, while the peripheral field of view illuminance was set at 100 lx ± 40%. Under these conditions, measurements were made for (1) the perceived transition from flicker (20 Hz) to light (60 Hz) and (2) the perceived transition from light (60 Hz) to flicker (20 Hz).
An increase in the flicker value before and after wearing the protector signified an improvement in eye strain, while a decrease in the flicker value indicated a worsening of eye strain.
Results
The flicker values for the ITY and N groups are presented in Figure 3-6 and Table 1. Throughout the study period, improvements in eye strain were observed as follows: 48.1% for subject A, 90.0% for subject B, 54.2% for subject C, 63.3% for subject D, 68.5% for subject E, 77.8% for subject F, and an overall improvement of 67.1% (p=0.0706965). Similarly, in the N group, the percentages were 37.2% for subject A, 82.1% for subject B, 53.4% for subject C, 63.4% for subject D, 74.1% for subject E, 70.4% for subject F, and an overall percentage of 64.1% (p=0.00845219). These results suggest a reduction in eye strain in the ITY group and a worsening of eye strain in the N group. When comparing the ITY group with the N group, improvements in eye strain were observed in all four patients in the ITY group. However, Pearson’s chi-square test (with Yates’ correction) for the entire group showed a p-value of 0.4989, indicating no significant difference.
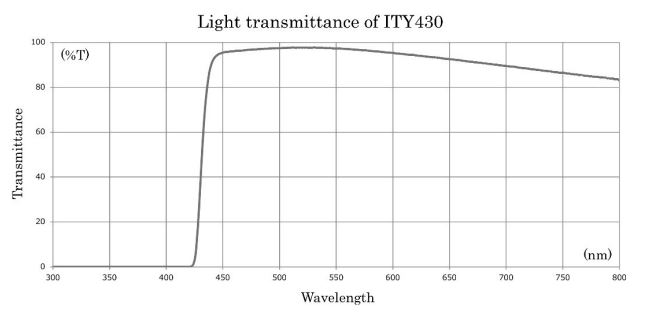
In comparison to multilayer film filters, this filter has a steeper inclination in the visible light spectrum, exhibits reduced dependency on the angle of incidence, and has minimal deviations in the ultraviolet cutoff wavelength.
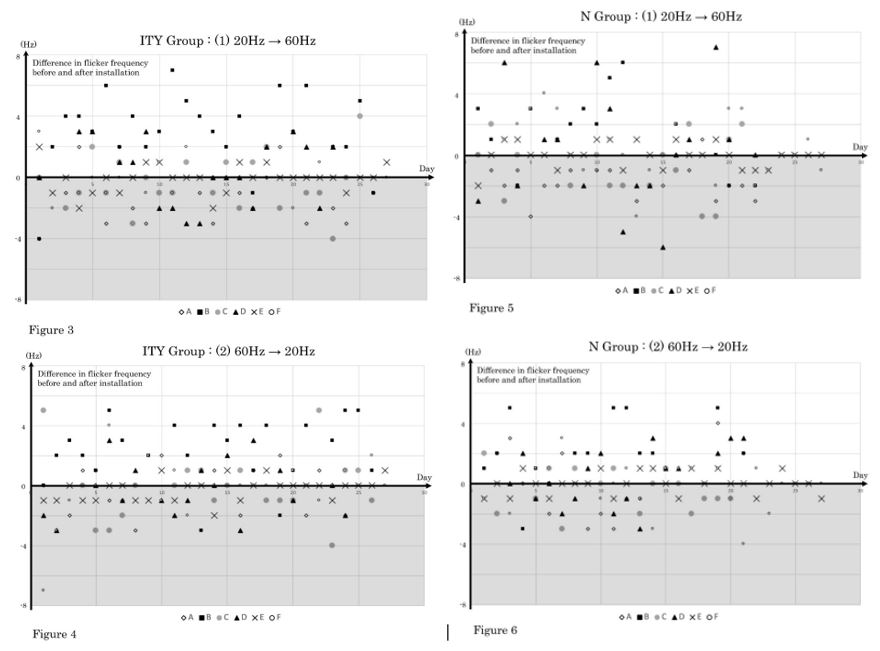
The vertical axis shows the difference in flicker values (Hz) before and after wearing the glasses, and the horizontal axis shows the date of the examination; the ITY group was wearing ITY430, and the N group wore glasses without b blue-violet light-cutting ability.
Figure 3 shows the measurement from 20 Hz to 60 Hz in the ITY430 group, whereas Figure 4 shows the measurement from 60 Hz to 20 Hz in the same group. Figure 5 shows the measurement from 20 to 60 Hz in the N group, and Figure 6 shows the measurement from 60 to 20 Hz in the N group. Positive flicker values indicate a reduction in eye strain, whereas negative values indicate an increase in eye strain.
Table 1: Summary of results from Figures 3-6.
| Subject | A | B | C | D | E | F | Total | ||
|---|---|---|---|---|---|---|---|---|---|
| ITY Group |
Eye strain | Improvement | 25 | 45 | 26 | 31 | 37 | 42 | 206 |
| (times) | Deterioration | 27 | 5 | 22 | 18 | 17 | 12 | 101 | |
| % improvement out of total | 48.1 | 90.0 | 54.2 | 63.3 | 68.5 | 77.8 | 67.1 | ||
| N Group |
Eye strain | Improvement | 16 | 32 | 21 | 26 | 40 | 38 | 173 |
| (times) | Deterioration | 27 | 7 | 18 | 15 | 14 | 16 | 97 | |
| % improvement out of total | 37.2 | 82.1 | 53.9 | 63.4 | 74.1 | 70.4 | 64.1 | ||
Discussion
In the dental practice setting, adequate illumination is essential for thorough examination of the oral cavity. LED light sources, in addition to indoor lighting, are often used in dental chair units, handpieces, microscopes, magnifying loupes, and electronic medical record displays. Blue LED light is used in irradiators to cure resins.
Light is a combination of three primary colors: red, green, and blue. White LEDs, which are increasingly prevalent indoors, exhibit emission peaks within the blue-violet light spectrum (400-490 nm) [1]. The amount of blue-violet light in a light source remains consistent across different technologies and is closely associated with the correlated color temperature [2].
t has been pointed out that the short wavelength, propensity for light scattering, and high energy of blue-violet light reaching the retina may potentially lead to photoreceptor cell damage [1]. Animal studies have shown that exposure to blue-violet light causes inflammatory apoptosis, DNA damage [3], and the generation of reactive oxygen species [4] in cells on the ocular surface and retina. Furthermore, it has been observed that various physiological functions may be affected [5], potentially impacting melatonin secretion, circadian rhythms, sleep patterns, and cognitive abilities [6].
Mixed results have been reported in human studies. Lin et al. reported reduced pain around and inside the eyes, diminished sensation of heaviness in the eyes, and less itching in the eyes when using blue-violet light-cut lenses following a two-hour computer work session [7]. In contrast, a study involving 120 subjects comparing blue-violet light blocking lenses with standard clear lenses revealed no significant difference in eye strain after a two-hour computer task [8]. Furthermore, Takashi et al. reported that the difference between the perceived eye strain and flicker values did not coincide [9].
These findings indicate disparities between results obtained at the cellular level and in animal experiments compared to outcomes when the lenses are worn by humans. Several factors should be considered, including the specific characteristics of blue-violet light blocking lenses, issues related to experimental conditions (e.g., the suitability of a 2 hour task duration), and the influence of variables other than the light source (e.g., working posture, blinking, etc.). The American Academy of Ophthalmology does not recommend blue-violet light cut glasses because of the lack of scientific evidence supporting the notion that blue-violet light is harmful to the eye [10]. In the POSITION STATEMENT ON THE BLUE LIGHT HAZARD published by The International Commission on Illumination in April, 2019 [11], it is noted that studies involving white light sources are unusual due to their in vitro experimental conditions, prolonged exposure periods, high color temperatures, fixed light sources, and exposures exceeding International Commission on Non-Ionizing Radiation Protection recommendations [12].
In its “Guidelines for Occupational Health Management in Information Equipment Work,” the Ministry of Health, Labor, and Welfare of Japan recommends that individuals working with Visual Display Terminals, such as liquid crystal displays and tablet terminals, limit their screen time to one hour and take a 10-15 minute break between consecutive working hours. The guideline also advocates for a 10-15-minute break between the continuous working periods and one or two short breaks within one continuous working period [13].
However, these guidelines primarily address issues related to eye strain caused by reduced blinking during prolonged screen use and do not directly refer to the effects of blue-violet light exposure.
When considering filters, it is worth noting that the ITY 430 offers certain advantages over multilayer options. This type of filter boasts a steeper gradient region for visible light, is less dependent on the angle of incidence and has a reduced wavelength shift to cut off ultraviolet light. It effectively blocks ultraviolet light while still allowing for a high degree of visible light transmittance. It has minimal impact on the perception of blueviolet colors. This particular type of glass has been patented in Japan under No. 5142139 and in the USA under US7951733B2 as “BLUE-VIOLET LIGHT BLOCKING GLASS.” We anticipate future research focusing on the effects of blue-violet light on eye strain. This study analyzed a large group of people who used the ITY430.
Conclusion
This study suggests that ITY430 has the potential to reduce eyestrain in dental practice. However, further case studies are required to assess its overall effectiveness.
Declarations
Acknowledgment: The findings of this study were presented at the 68th Annual Meeting of the Japanese Society of Oral and Maxillofacial Surgery (8-11 November 2023, Osaka). We would like to thank Editage (www.editage.jp) for English language editing.
Competing interests: The authors state no conflicts of interest regarding this study.
References
- C Stamatacos, J L Harrison. The possible ocular hazards of LED dental illumination applications. J Tenn Dent Assoc. 2013; 93: 25-29.
- S J Dain. The blue light dose from white light emitting diodes (LEDs) and other white light sources. Ophthalmic Physiol Opt. 2020; 40: 692-699.
- X Ouyang, J Yang, Z Hong, Y Wu, Y Xie, G Wang. Mechanisms of blue light-induced eye hazard and protective measures: a T review. Biomed Pharmacother. 2020; 130: 110577.
- F Yoshino, A Yoshida. Effects of blue-light irradiation during dental treatment. Jpn Dent Sci Rev. 2018; 54: 160-168.
- G Tosini, I Ferguson, K Tsubota. Effects of blue light on the circadian system and eye physiology. Mol Vis. 2016; 24: 61-72.
- S Wahl, M Engelhardt, P Schaupp, C Lappe, I V Ivanov. The inner clock-Blue light sets the human rhythm. J Biophotonics. 2019; 12: 201900102.
- J B Lin, B W Gerratt, C J Bassi, R S Apte. Short-Wavelength LightBlocking Eyeglasses Attenuate Symptoms of Eye Fatigue. Invest Ophthalmol Vis Sci. 2017; 58: 442-447.
- Singh, L E Downie, A J Anderson. Do Blue-blocking Lenses Reduce Eye Strain From Extended Screen Time? A Double-Masked Randomized Controlled Trial. Am J Ophthalmol. 2021; 226: 243-251.
- T Ide, I Toda, E Miki, K Tsubota. Effect of Blue Light-Reducing Eye Glasses on Critical Flicker Frequency. Asia Pac J Ophthalmol (Phila). 2015; 4: 80-85.
- American Academy of Ophthalmology: Are Blue Light-Blocking Glasses Worth It? 2023. https://www.aao.org/eye-health/tipsprevention/are-computer-glasses-worth-it.
- The International Commission on Illumination, POSITION STATEMENT ON THE BLUE LIGHT HAZARD. 2019.
- ICNIRP Guidelines on Limits of exposure to incoherent visible and infrared radiation. Health Phys. 2013; 105: 74-96.
- Ministry of Health, Labour and Welfare: guidelines for occupational health management in information equipment work. 2022. Available at https://www.mhlw.go.jp/content/000539604.pdf; (Accessed 11 Nov 2023).