SciBase Journals
SciBase Dentistry and Oral Sciences
- Article Type: Research Article
- Volume 2, Issue 2
- Received: Aug 14, 2024
- Accepted: Oct 02, 2024
- Published Online: Oct 09, 2024
Clinical Assessment of Hyperbaric Oxygen Combined with PRF on the Effects of Gingival Papillae Loss and Periodontal Bone Defects: A Case-Control Study
Tie-Lou Chen1,2*; Hui-Jie Lu3; Ting-Lin Zhang4; Bing Xu5; Dong-Sheng Xu6; An-Xin Yue7; Yi-Yi Pang8; Yan-En Wang1; Chuan-Mei Huang1s; Zhi-Zen Quan1; Xin-Yu Yang1; Shi-Feng Wang9*; Da-Hai Tang10*; Yi-Jun Zhou11*
1Department of Periodontology, Stomatology Center of the First Affiliated Hospital of Naval Medical University, National Stomatology Medical Center Periodontology Specialty Alliance Unit, Shanghai 200081, China
2Key Laboratory of Hyperbaric Oxygen Medicine and Physiology of the PLA, Shanghai 200433, China.
3Department of Aerospace Medicine, Air Force Medical University, 710032, China.
4Clinical Research Center, the First Affiliated Hospital of Naval Medical University, Shanghai 200081, China.
5Department of Chemistry, Chemical College, Tongji University, Shanghai, 200092, China.
6Department of Stomatology, Baoshan Branch of Shanghai University of Traditional Chinese Medicine Affiliated Shuguang Hospital, Baoshan District Central Hospital, Shanghai, 201999, China.
7Department of Stomatology, Affiliated Hospital of Dalian Medical University, Dalian, China.
8Comprehensive Department of Hangzhou Stomatological Hospital, Hangzhou, 310013, Chian.
9Key Laboratory of Hyperbaric Oxygen Medicine and Physiology of the PLA, Naval Medical University, Shanghai 200433, China.
10Clinical Laboratory Department, the First Affiliated Hospital of Naval Medical University, Shanghai 200081, China.
11Department of Periodontology, State Key Laboratory of Military Stomatology & National Clinical Research Center for Oral Diseases & Shaanxi Clinical Research Center for Oral Diseases, School of Stomatology, Fourth Military Medical University, Xi’an, 710032, China.
#Tie-Lou Chen, Hui-Jie Lu and Ting-Lin Zhang are co-first authors.
*Corresponding Author: Tie-Lou Chen1, Shi-Feng Wang2, Da-Hai Tang3
& Yi-Jun Zhou4
1Department of Periodontology, Stomatology Center of the First Affiliated
Hospital of Naval Medical University, National Stomatology Medical Center
Periodontology Specialty Alliance Unit, Shanghai 200081, China.
2Key Laboratory of Hyperbaric Oxygen Medicine and Physiology of the
PLA, Naval Medical University, Shanghai 200433, China.
3Clinical Laboratory Department, the First Affiliated Hospital of Naval
Medical University, Shanghai 200081, China.
4Department of Periodontology, State Key Laboratory of Military
Stomatology & National Clinical Research Center for Oral Diseases &
Shaanxi Clinical Research Center for Oral Diseases, School of Stomatology,
Fourth Military Medical University, Xi’an, 710032, China.
Email: chentielou2010@163.com, 156362518@qq.com, tdh863@163.com, zhouyijunyzk@163.com
Abstract
Objective: To investigate the clinical effects of Hyperbaric Oxygen Therapy (HBO) combined with Platelet-Rich Fibrin (PRF) on the treatment of gingival papillae loss and periodontal bone defects.
Methods: 150 cases of chronic periodontitis patients with gingival papillae loss and periodontal bone defects were selected and divided into three groups after calcined bone grafting: the HBO-PRF group, the PRF group, and the control group, with 50 cases in each group. The Gingival Index (GI), Periodontal Pocket Depth (PD), and Clinical Attachment Loss (AL) were recorded before surgery and at 6 and 12 months post surgery. Gingival papillae height (GPH) and black triangles area (BTA) of the experimental teeth were measured before treatment and at 12 months post-treatment using a digital single-lens reflex camera.The Keratinized Gingival Width (KGW) was measured at different time points. The CBCT and periapical X ray were taken to measure the bone density and bone filling, and the rate of bone improvement was calculated.
Results: The HBO-PRF group showed significantly reduced of the GI, PD, and AL at 6 and 12 months post surgery compared to the PRF group and the control group. The improvements in GPH and BTA in the HBO-PRF group were markedly better than those in the PRF group and control group. The reduction in KGW was significantly lower than that of the PRF group at 1, 3, 6, and 12 months post surgery. The HBO-PRF group had a significantly higher bone density and bone fill improvement at 6 and 12 months compared to the PRF group and the control group.
Conclusion: HBO combined with PRF can significantly increase the GPH and KGW, reduce the BTA, promote periodontal bone regeneration, and have significant therapeutic effects on the gingival papillae loss and the repair of periodontal bone defects.
Keywords: Hyperbaric oxygen; Platelet-rich fibrin; Keratinized gingival width; Black triangles area; Gingival papillae loss; Periodontal bone defect/regeneration.
Citation: Tie-Lou Chen, Hui-Jie Lu, Ting-Lin Zhang, et al. Clinical Assessment of Hyperbaric Oxygen Combined with PRF on the Effects of Gingival papillae loss and Periodontal Bone Defects: A Case-Control Study. SciBase Dent Oral Sci. 2024; 2(2): 1015.
Introduction
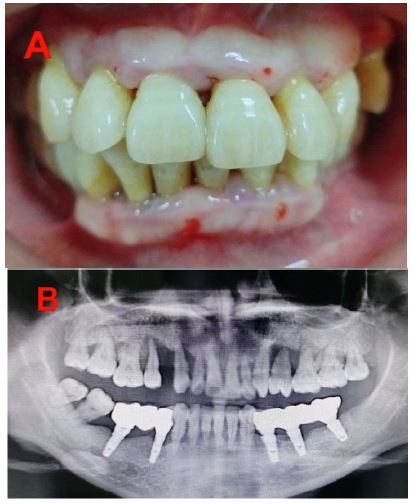
Gingival recession and periodontal bone defects are the most common problems in oral symptoms, and are the main cause of tooth loss, which seriously affects patients’ aesthetics and chewing function (Figure 1). Traditional treatment methods such as flap curettage, gingival grafts and bone defects filling are effective but have certain limitations, such as long healing time, poor bone regeneration ability, and many complications. In recent years, Platelet-Rich Fibrin (PRF), as an autologous platelet concentrate, has attracted widespread clinical attention due to its high con- centration of platelets, growth factors, and fibrinogen, which significantly promote the tissue regeneration and repair of soft and hard tissues. The preparation method of PRF is simple, rich in growth factors, and free from immune reactions, therefore it has garnered widespread attention in clinical practice [1,2]. Previous studies have confirmed that the combination of PRF with artificial bone can improve the total effective rate and new bone formation [3].
Systematic reviews by Miron RJ have found that PRF has advantages in promoting bone regeneration and reducing complications in the repair of periodontal bone defects [4,5]. In addition, Hyperbaric Oxygen Therapy (HBO) can enhance cell metabolism and repair ability by increasing tissue oxygen concentration, playing an important role in promoting soft tissue growth, wound healing and bone regeneration [6].
However, there are few reports on the control study of HBO combined with PRF in the repair of gingival papillae loss and periodontal bone defects. Therefore, the application of HBO in combination with PRF may provide a new and effective treatment strategy for the repair of gingival papillae loss and periodontal bone defects. Based on this, further research on the role of HBO combined with PRF in the repair of interdental papilla loss and periodontal bone defects of periodontal patients has important clinical significance and theoretical value.
Materials and methods
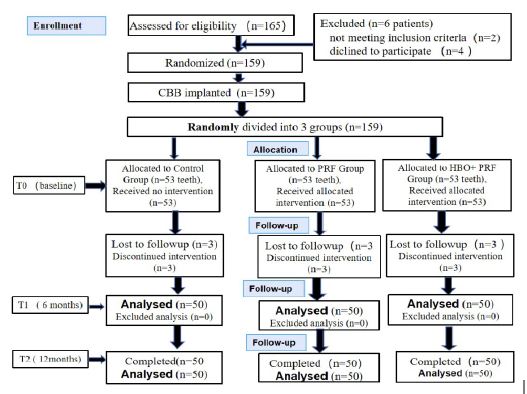
Patient selection: 159 patients with severe chronic periodontitis who met the inclusion criteria for this experiment were selected from those visiting the Stomatology Center of Changhai Hospital, Naval Medical University (one tooth was chosen per patient as the subject of the study, meeting the conditions for bone grafting). There were 79 male and 80 female patients, aged 38 to 61 years (average 48.5 years old). All patients underwent debridement and implantation of Calcined Bovine Bone (CBB) on the basis of periodontal basic treatment. According to the experimental design, patients were randomly divided into three groups: the HBO-PRF group, the PRF group, and the control group, with 53 cases in each group (Figure 2). This study was approved by the Ethics Committee of Changhai Hospital, Naval Medical University, and the patients signed informed consent forms.
Inclusion criteria: At the one-month follow-up after periodontal basic treatment, there should be at least one quadrant in the oral cavity with a periodontal pocket depth (PD)≥6 mm and a loss of periodontal attachment (AL)≥3 mm, and X- ray examination should show a clear infrabony pocket (grade 2 or higher bone absorption). Platelet count is greater than 100×109/L.
Exclusion criteria: Patients with severe systemic diseases, women in pregnancy or lactation, those who have taken medication affecting platelet function within 3 months before surgery, and patients with smoking and alcohol abuse.
Preparation of PRF: At 0.5 hours before surgery, 5 mL of venous whole blood was quickly drawn using a sterile vacuum glass tube (without anticoagulant), and immediately placed in a TLXJ-IIC centrifuge (An Ting Scientific Instrument Factory, Shanghai, China). It was then centrifuged at 3000 r/min for 10 minutes (with a centrifugal radius of 10 cm), and left to stand for 3 to 5 minutes. At this time, the centrifuge tube is divided into three layers: The uppermost layer is the supernatant, the lowest layer is the red blood cell layer, and the middle yellowish gel layer is the PRF. After centrifugation, the centrifuge tube is placed in a 37°C water bath for later use.
Treatment plan: Under local anesthesia, a full-thickness flap procedure was performed, the flap was raised to expose the bone defect area, and after debridement and root surface planing, the root surface was treated with minocycline for 3 minutes, followed by rinsing with saline. According to the experimental design, patients were divided into three groups (Figure 2).
HBO-PRF group: PRF was pressed into a membrane using sterile gauze, evenly divided into two parts, one part was prepared into fragments and mixed with the bone graft particles of CBB (Shaanxi, Ruisheng Biotechnology Co., Ltd., production batch number: 161202) and filled into the bone defect, the other PRF membrane was placed on the surface of the transplanted bone powder, the flap was repositioned and sutured, and the wound was dressed, starting from the second day after surgery, the patient received 0.25 MPa HBO exposure for 1 hour a day, five times a week, for a total of two weeks.
PRF group: CBB particles were implanted into the bone defect area, covered with a PRF membrane, and the wound was sutured.
Control group: After implanting CBB particles, the wound was sutured. Sutures were removed two weeks after surgery, and no periodontal probing was performed within six months after surgery. The patient took oral cefaclor capsules 0.5 g and metronidazole tablets 0.4 g, three times a day for one week, used Xipayi Guyin liquid (Xinqikang Pharmaceutical Co., Ltd.) for mouth rinsing, 3 ml each time, three times a day, for six weeks, and avoided biting hard objects in the surgical area within four weeks.
Clinical indicator measurements: Periodontal clinical parameters were assessed at baseline, and at 6 and 12 months after surgery by two calibrated clinicians with a high level of agreement (κ>0.80) when collecting periodontal parameters. The following parameters were measured:
(1) The Gingival Index (GI) [7], which assesses the inflammation of the gingiva. (2) Probing Depth (PD), measured from the free gingival margin to the bottom of the pocket using a periodontal probe (Hu-Friedy Manufacturing, Chicago, IL, USA). (3) Attachment Loss (AL), measured from the enamel-cemental junction to the bottom of the pocket using a periodontal probe. GI, PD and AL were recorded at six sites per tooth (mesio-buccal, buccal, disto-buccal, disto-lingual, lingual, and mesio-lingual) around the teeth under investigation [8].
Measurement of gingival papilla height and black triangle area: Digital photographs of the gingival papilla recession sites of the experimental teeth were taken before treatment and at 12 months post-treatment using a digital single-lens reflex camera. The camera lens was positioned perpendicular to the labial surface of the long axis of the target tooth for the photograph. The photographs were then imported into the Digimizer version 4.2 software (MedCalc Software, Belgium). The software’s line length calibration function was used to measure distances and areas based on the clinical photographs. The baseline was drawn from the Cervical Cemento-Enamel Junction (CEJ) of the adjacent teeth on the mesial and distal sides of the target gingival papilla (or the gingival margin instead) to the highest point on the root side, and a perpendicular line was drawn from the highest point of the gingival papilla to the baseline, indicating the Gingival Papilla Height (GPH) value. The image of the scale ruler in the photograph was used to calibrate the numerical value (principle: by clicking the calibration button and selecting two points on the ruler with a 10 mm interval, set the distance as 10 mm in the pop-up box. Then click on any two endpoints of a line segment, and the software’s data measurement list will display the corresponding length value for this distance). The Black Triangle Area (BTA) was outlined, and the area was auto- matically calculated by the software (Figure 3). Two examiners separately calculated the actual GPH and the BTA, and the average values were taken [9].
Measurement of keratinized gingival width: The KGW at the central buccal aspect of the experimental teeth in the surgical area was measured using a periodontal calibrated probe before surgery, and at 2 weeks, and 1, 3, 6, and 12 months post operation. Each site was measured twice, and the average value was taken. The reduction of KGW= (the pre-operative KGW) - (the post-operative KGW).
Bone density assessment: Cone Beam Computed Tomography (CBCT, i-CAT 17- 19, Kavo, USA) was performed before surgery and at 6 and 12 months post operation. Bone density (BD) in the grafted area was measured using the iCATVision software (Version 1.9.3.14, USA) and expressed in Hounsfield Units (HU).
Bone filling height measurement and comparison of bone improvement degree: X-ray films of the experimental teeth were taken, and the X-ray images of the experimental teeth were imported into a computer, then transferred to the Digimizer version 4.2 software (MedCalc Software, Belgium). Set the length of the tooth in the image to 10 (unit), The alveolar bone filling height (BFH) of each group was measured using the Digimizer 4.2 Image Program software before surgery and at 6 and 12 months post- surgery (Figure 4). The improvement rate of the BFH of the experimental teeth at 12 months was calculated according to the following formula, and the results were categorized as:
(1) mild improvement, where the change of alveolar bone height is less than 50%;
(2) moderate improvement, where the alveolar bone height increases by more than 50% but less than 150%;
(3) significant improvement: where the alveolar bone height increases by more than 150%. The alveolar bone height expressed in units (u).
The formula is as follows:
Alveolar BFH Improvement Rate= (Bone Height at 12 Months Post therapy - Pre therapy Bone Height) ÷(Pre therapy Bone Height) ×100%.
BFH Significant Improvement Rate= (Number of Moderate Improvement Cases + Number of Significant Improvement Cases) ÷(Total Number of Cases) ×100%.
Statistical analysis: The data were statistically analyzed using IBM SPSS 23.0 (IBM Corp., Armonk, NY, USA). The outcome assessment and data analysis were performed by individuals blinded to group assignment information. The outcome assessment and data analysis were carried out by an author blinded to the group allocation information. Results were presented in the form of mean ± standard deviations. We used one-way ANOVA in combination with Paired t-test, independent samples t-test, Chi-Square Test and rank sum test (Wilcoxon) to compare the difference of multiple groups. Statistical significance was set at p<0.05.
Results
A total of 159 patients in this group completed the clinical surgery. Among them, in the HBO-PRF group of 53 cases, 1 case did not complete HBO treatment, and 2 cases were lost to follow-up. In the PRF group of 53 cases, 3 cases were lost to follow-up, and in the Control group of 53 cases, 1 case had postoperative infection, which improved after treatment with metronidazole tablets and cefaclor capsules and was subsequently withdrawn from the experiment, and 2 cases were lost to follow-up. 150 cases in this study completed the clinical research and data analysis.
Comparison of periodontal clinical indices: In the HBO-PRF group, GI, PD, and AL were significantly reduced compared to the PRF group at 6 and 12 months postoperatively. The PRF group showed significant differences in GI, PD, and AL compared to the Control group at 6 and 12 months postoperatively (Table 1).
Comparison of the GPH and BTA: Among Groups at 12 months after surgery, both the HBO-PRF group and the PRF group showed a significant increase in GPH and a significant reduction in BTA compared to the control group. The improvements in GPH and BTA in the HBO-PRF group were markedly better than those in the PRF group (Table 2).
Comparison of keratinized gingival width: The reduction of KGW in the HBO-PRF group and the PRF group were significantly less than those in the Control group at 1, 3, 6, and 12 months postoperatively. There were significant differences in the reduction of KGW at 3, 6, and 12 months compared to 1 month postoperatively, and no significant differences in the reduction of KGW at 6 and 12 months compared to 3 months postoperatively. The reduction of KGW in the HBO-PRF group were significantly less than those in the PRF group at 1, 3, 6, and 12 months (Table 3).
Bone density comparison: At 6 and 12 months post-operation, there were significant differences in bone density (BD) among the three groups compared to pre-operative levels. The BD in the HBO-PRF group was significantly higher compared to the PRF group and the Control group at 6 and 12 months post-operation. The HBO-PRF group showed a marked increase in BD at 6 and 12 months compared to the PRF group (Table 4).
Comparison of bone fill improvement efficacy: The HBO- PRF group showed a significantly greater bone fill height (BFH) at 6 and 12 months post-operatively compared to the PRF group and the Control group, with the PRF group also showing a significant greater BFH over the Control group (Table 5).
At 12 months after surgery, in the HBO-PRF group of 50 cases, the number of cases with BFH improvement was 47, which accounts for 94%, a proportion significantly higher than that of the PRF group (28%). The BFH significant improvement rate of HBO-PRF group (100%) was also significantly higher than that of the PRF group (88%) and the Control group (14%) (Table 6).
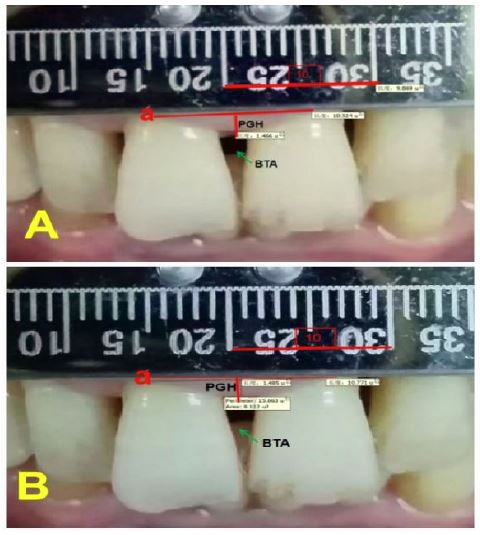
Abbreviations: BTA: Black Triangles Area; GPH: Gingival Papilla Height; a: the line connecting the CEJ on the labial surface of adjacent teeth; u: Units.
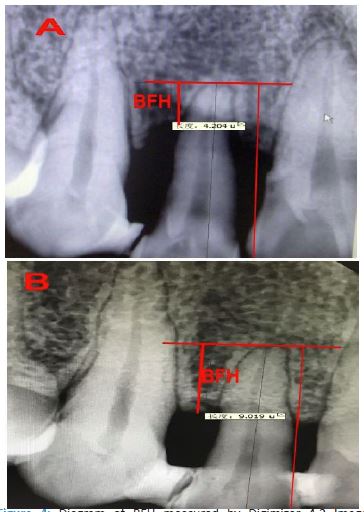
Table 1: Comparisons of the GI, PD and AL between groups at baseline, 6 and 12 months ♦
| Groups | n | GI | PD(mm) | AL(mm) |
|---|---|---|---|---|
| Control | ||||
| baseline | 50 | 1.95 ± 0.30 | 6.60± 1.30 | 6.75 ± 1.10 |
| 6M post-therapy | 50 | 0.93± 0.40** | 3.81± 1.10** | 5.25± 1.05* |
| 12M post-therapy | 50 | 1.05± 0.41** | 3.78± 1.05** | 5.35± 1.00* |
| PRF | ||||
| baseline | 50 | 1.90 ± 0.42 | 6.51± 1.20 | 6.70 ± 1.30 |
| 6M post-therapy | 50 | 0.65± 0.25**# | 2.80± 1.00**# | 3.20± 0.50**# |
| 12M post-therapy | 50 | 0.63± 0.15**# | 2.71± 1.05**# | 3.01± 0.65**# |
| HBO-PRF | ||||
| baseline | 50 | 1.93 ± 0.33 | 6.53± 1.30 | 6.67 ± 1.30 |
| 6M post-therapy | 50 | 0.35± 0.13**##$ | 2.05 ± 0.25**##$ | 2.60± 0.32**##$ |
| 12M post-therapy | 50 | 0.33± 0.10**##$ | 1.88 ± 0.35**##$ | 2.50± 0.40**##$ |
Significant differences compared with baseline, *P< 0.05, **P< 0.01. Significant differences compared with Control group,# p< 0.05, ## p< 0.01. Significant differences compared with PRF group, $ P < 0.05.
♦ Numbers are mean ±standard deviations.
Abbreviations: HBO: hyperbaric oxygen; PRF: platelet rich fibrin; GI:gingival index; PD:probing depth; AL:attachment loss; M: month.
Table 2: Comparison of the GPH and BTA between groups at baseline and 12 months post-therapy ♦
| Groups | GPH (u) | BTA (u2) | ||
|---|---|---|---|---|
| Baseline | 12M post-therapy | Baseline | 12M post-therapy | |
| Control | 3.41±0.25 | 3.37±0.30 | 1.25±0.13 | 1.28±0.19 |
| PRF | 3.48±0.30 | 3.79±0.28* | 1.30±0.11 | 0.99±0.10* |
| HBO-PRF | 3.40±0.25 | 4.10±0.20**# | 1.24±0.10 | 0.87±0.11**## |
Significant differences compared with Control group, * p< 0.05, ** p< 0.01. Significant differences compared with PRF group, # p< 0.05, ## p< 0.01. ♦ Numbers are mean ±standard deviations.
Abbreviations: HBO: hyperbaric oxygen; PRF: platelet rich fibrin; M: month; GPH:Gingival papilla height; BTA: black triangle area; u: units.
Table 3: Comparison of the KGW changes between groups at different time points ♦
| Groups | Different time points post-therapy | ||||
|---|---|---|---|---|---|
| 2 W | 1M | 3M | 6M | 12M | |
| Control | 0.45±0.25 | 1.35±0.30 | 1.39±0.35 | 1.42±0.45 | 1.41±0.40 |
| PRF | 0.36±0.15 | 0.69±0.40* | 0.82±0.30*$ | 0.83±0.40*$ | 0.84±0.25*$ |
| HBO-PRF | 0.25±0.10 | 0.45±0.15**# | 0.59±0.15**#$ | 0.60±0.30**#$ | 0.61±0.15**#$ |
Significant differences compared with Control group, * p< 0.05, ** p< 0.01. Significant differences compared with PRF group, # p< 0.05. Significant differences compared with 1 month post-therap, $ P < 0.05. ♦ Numbers are mean ±standard deviations.
Abbreviations: HBO: hyperbaric oxygen; PRF: platelet rich fibrin; KGW: keratinized gingival width; M: month; W: week.
Table 4: Comparison of the BD between groups at different time points (HU) ♦
| Groups | Different time points | ||
|---|---|---|---|
| baseline | 6Mpost-therapy | 12M post-therapy | |
| Control | 130.10±10.50 | 601.50±25.30 | 580.60±15.40 |
| PRF | 133.20±15.10 | 669.60±17.40* | 671.50±19.10* |
| HBO-PRF | 125.45±12.50 | 725.50±30.25**# | 734.40±15.3**# |
Significant differences compared with Control group, * p< 0.05, ** p< 0.01. Significant differences compared with PRF group, # p< 0.05. ♦ Numbers are mean ±standard deviations.
Abbreviations: HBO: hyperbaric oxygen; PRF: platelet rich fibrin; BD:bone density; M: month.
Table 5: Comparison of the BFH between groups at different time points (u) ♦.
| Groups | Different time points | ||
|---|---|---|---|
| baseline | 6Mpost-therapy | 12Mpost-therapy | |
| Control | 1.15±0.01 | 1.83±0.08 | 1.71±0.10 |
| PRF | 1.22±0.02 | 3.48±0.10** | 3.10±0.15* |
| HBO-PRF | 1.25±0.01 | 5.35±0.15**## | 5.12±0.13**## |
Significant differences compared with Control group, * p<0.05, ** p<0.01. Significant differences compared with PRF group, ## p<0.01. ♦ Numbers are mean ±standard deviations.
Abbreviations: HBO: hyperbaric oxygen; PRF: platelet rich fibrin; BFH: bone filling heights; M: month; u: units.
Table 6: Comparison of the efficacy of bone filling improvement at 12 months between groups.
| Groups | Total number | Cases number of bone filling improvement at 12M post-therapy (%) | ||
|---|---|---|---|---|
| Mildimprovement | Moderate improvement | Severe improvement | ||
| Control | 50 | 43 (86%) | 7 (14%) | 0(0%) |
| PRF | 50 | 6 (12%) | 30 (60%)** | 14(28%)** |
| HBO-PRF | 50 | 0 (0%) | 3 (6%)**## | 47 (94%)**## |
Significant differences compared with Control group, ** p< 0.01. Significant differences compared with PRF group, ## p< 0.01.
Abbreviations: HBO: hyperbaric oxygen; PRF: platelet rich fibrin; M: month.
Discussion
Periodontal soft and hard tissue regeneration has always been a challenging and hot topic in the treatment of periodontitis. PRF, as a second-generation autologous platelet concentrate containing cells, growth factors, and fibrin bio-scaffolds, has seen changes in its biological characteristics due to the development of low-speed centrifugation techniques. These changes make PRF closer to the ideal tissue regeneration system in terms of biosignaling molecules and bio-scaffolds, promoting vascular regeneration and tissue healing. The combined application of PRF with other technologies can better promote periodontal tissue regeneration. Because it is easy to obtain and cost-effective, PRF has been applied in the treatment of periodontal soft and hard tissue regeneration in recent years [10]. Systematic reviews have shown that PRF is significantly effective in the treatment of periodontal intrabony defects, and the efficacy of PRF combined with flap surgery is better than that of bone grafting alone [4]. Since platelets in PRF can activate and release growth factors to stimulate the proliferation and differentiation of mesenchymal stem cells from bone marrow, promoting collagen synthesis, and the three-dimensional fibrin network structure is beneficial to the migration of fibroblasts and osteoblasts and new bone formation [11]. In vitro experiments have found that PRF can promote cell proliferation and differentiation, and the regeneration of soft and hard tissues, and platelets in PRF can slowly release growth factors for up to 28 days [12]. Animal experiments have confirmed that PRF combined with Periodontal Ligament Cells (PDLC) can promote periodontal tissue regeneration in rats [13]. Clinical studies have found that PRF combined with hydroxyapatite has a certain curative effects on human periodontal bone defects [14] and promotes the healing of periodontal soft tissue defects [15]. Electron microscopy confirmed that the collagen fibers in PRF are arranged in a loose and porous network structure, containing a large number of stationary or activated platelets and white blood cells located between collagen fibers [16]. This structure can promote vascular and tissue regeneration, and white blood cells have anti-infection effects, which are beneficial to tissue healing. The findings of this study show that the GI, PD, and AL in the PRF group were significantly improved at 6 and 12 months post-operation compared to the control group, indicating that PRF has a significant therapeutic effects on the clinical efficacy of periodontitis.
The gingival papilla loss or gingival papilla recession leading to black triangle is a challenging issue in the treatment of periodontitis, and currently there is a lack of effective treatment methods. This study found that at 12 months post-operation, both the HBO-PRF group and the PRF group had significantly higher GPH and significantly reduced BTA compared to the control group. This is related to the activation and release of a large number of growth factors and the fibrin scaffold structure by PRF [17]. The anti-inflammatory and tissue regeneration promoting effects of HBO may have played a role in the post operative regeneration of the gingival papilla [18-19]. These results are consistent with the findings reported by Awartani FA [20].
Regarding the role of PRF in gingival recession, Aroca S et al. [21] showed that PRF can improve the thickness of keratinized gingiva and the level of periodontal attachment in patients with gingival recession. At 12 months, the root coverage rate in the PRF group was similar to that of the connective tissue graft group, indicating that PRF can be used as an alternative to connective tissue grafting in the treatment of gingival recession [22]. The present study found that at 1, 3, 6, and 12 months post-operation, the reduction of KGW in the PRF group were significantly less than those in the control group. The reduction of KGW at 6 and 12 months were similar to those at 3 months, suggesting that the effect of PRF on KGW becomes stable by 3 months post-operation. This is consistent with the theory that growth factors in PRF are continuously released.
Animal experiments have demonstrated that Platelet-Rich Plasma (PRP) combined with bone graft materials can promote the repair of bone defects [23]. PRF combined with PDLC and Mesenchymal Stem Cells (MSCs) facilitates the formation of periodontal tissue in nude rats [24]. The bFGF secreted by PRF, when combined with CBB, has good therapeutic effects on periodontal bone regeneration [25]. The present study found that at 6 and 12 months post-operation, the bone density in the PRF group was significantly better than that in the control group. At 12 months, the bone filling height in both the PRF group and the HBO-PRF group was significantly better than that in the control group, consistent with the results of Sharma A [26].
Although PRF (PRF) has shown good effects on periodontal tissue and hard tissue defects, the difficulty in bone regeneration efficacy is due to the anaerobic bacterial infection and the anatomical characteristics of periodontitis. Therefore, the research on the combination of PRF with other technologies to promote the soft and hard tissue regeneration is of great significance. This clinical study adopted the treatment of gingival papillae loss and periodontal bone defects with PRF combined with HBO. The results showed that at 6 and 12 months post-operation, the GI, PD, and AL in the HBO-PRF group were significantly improved compared to the PRF group. The bone density, bone filling height showed significantly improved, which were better than those in the PRF group, and consistent with the results of Johannes [27]. The therapeutic effect of HBO is related to its ability to improve the osteogenic and angiogenic effects of bone marrow mesenchymal stem cells under inflammatory conditions in vitro [28]. In addition, it is also related to the increased expression of Runx2 by HBO, which promotes calcium salt deposition and accelerates the formation of new bone [29].
There are relatively few reports on the mechanisms by HBO promotes gingival and bone regeneration. Izumino J found that HBO has a therapeutic effect on rats with cranial defects because it promotes the expression of basic Fibroblast Growth Factor (bFGF) in the early stages [30]. HBO can promote angiogenesis and the expression of Vascular Endothelial Growth Factor (VEGF) in animal bone defects, positively regulating tissue healing [31]. In addition, HBO can stabilize and activate hypoxia-inducible factor 1 (HIF- 1), increase cell proliferation, and improve wound healing in animals [32].
Our previous studies have confirmed that the combination of HBO and bFGF has a significant synergistic effect on the healing of rat bone defects, and this is related to the regulation of the expression of OPG and CD34 [33]. This study indicated that there were significant synergistic effects of HBO combing PRF on gingival papilla loss and periodontal bone defects. However, further research with a larger sample size is needed to elucidate the clinical effects and detailed mechanism.
Conclusion
The combination of HBO and PRF can significantly enhance the efficacy of CBB in repairing the loss of gingival papilla and periodontal bone defects. It can also increase GPH and KGW, reduce the area of black triangles, enhance the level of periodontal attachment, and promote the regeneration of periodontal bone. Its effectiveness is related to HBO’s ability to elevate oxygen levels within gingival tissue, regulate HIF-1α, and improve microcirculation, as well as PRF’s richness in growth factors and scaffold structures. This study provides a new and effective treatment method for the repair of interdental papilla loss, insufficient keratinized gingiva, and periodontal bone defects.
Abbreviations: HBO: Hyperbaric Oxygen; PRF: Platelet- Rich Fibrin; CBB: Calcined Bovine Bone; GI: Gingival Index; PD: Probing Depth; AL: Attachment Loss; CBCT: Cone-Beam Computed Tomography; ELISA: Enzyme-Linked Immunosorbent Assay; OPG: Osteoprotegerin; RANKL: Receptor Activator of Nuclear Factor-Kb Ligand; GCF: Gingival Crevicular Fluid; KTW: Keratinized Gingival Width; PRP: Platelet-Rich Plasma; bFGF: Basic Fibroblast Growth Factor; VEGF: Vascular Endothelial Growth Factor; HIF: Hypoxia-Inducible Factor; GPH: Gingival Papilla Height; BTA: Black Triangle Area; BD:bone density;BFH: bone filling heights;U: Units; M: Months.
Declarations
Acknowledgements
The authors thank Professor Xiaoxi Wang and Si Xu for their help in biological marker determination. We would like to thank Wenjing Chen, Xuelan Sun, Xianhui Wu,Caidi Jiang, Ziyan Guo, Liting Ma, Zhaoze Ma,Yifan Zhang, Baishun Chen and Zengnan Shan for their help in clinical observation. The study was supported by Shanghai Municipal Health and Family Planning Commission Scientific Research Project (20134418) and General Logistics Department Project (CHJ13J035). This study is also funded by 234 discipline peak climbing projects (2020YXK028) and education reform projects (CHJG2020040) and 2023 Basic Medical Research Project (2023PY09) of the First Affiliated Hospital of Naval Medical University, and Shanghai Science and Technology Major Project (No. 2023SHZDZX02-030702).
Conflict of interest: No conflicts of interest relevant to this article.
References
- Miron RJ, Zucchelli G, Pikos MA, Salama M, Lee S, et al. Use of platelet- rich fibrin in regenerative dentistry: A systematic review. Clin Oral Investig. 2017; 21: 1913- 1927.
- Kang YH, Jeon SH, Park JY, Chung JH, Choung YH, et al. Platelet-rich fibrin is a bioscaffold and reservoir of growth factors for tissue regeneration. Tissue Eng Part. A. 2011; 17: 349-359.
- Zhang J, Xia CC, Li XP. Clinical application of Platelet-Rich Fibrin (PRF) combined with artificial bone meal in oral implant-guided bone regeneration. Chinese Journal of Oral Implantology. 2020; 25: 165-168.
- Miron RJ, Moraschini V, Fujioka-Kobayashi M, Zhang Y, Kawase T, et al. Use of Platelet-Rich Fibrin in the Treatment of Periodon- tal Intrabony Defects: A Systematic Review and Meta-Analysis. Biomed Res Int. 2021; 2021: 6669168.
- Ning Ye, Tang Liyu, Gong Feifei, Zhuang Shaoyu, Xia Huakuan. Ef- fects of platelet-rich fibrin combined with Bio-Oss bone substitute in the repair of postoperative bone defect of jaw cyst. Journal of Bengbu Medical University. 2024; 49: 187-191.
- Chen Tie-lou, Xu Bing, Liu Jingchang, Li Shuguang, Li Deyi, et al. Effects of hyperbaric oxygen on aggressive periodontitis and sub- gingival anaerobes in Chinese patients [J]. J Indian Soc Periodon- tol. 2012; 16: 492-497.
- Loe H. The gingival index, the plaque index and the retention in- dex systems. J Periodontol. 1967; 38: 610-616.
- Ramfjord SP. Indices for prevalence and incidence of periodontal disease. J Periodontol. 1959; 30: 51-59.
- Wu Chunlan, Zhou Zichao, Liu Anhao, Shu Rong, Li Chaolun. Clini- cal evaluation of reconstruction of interdental papilla with hyal- uronic acid gel. Stomatology. 2018; 38: 48- 51.
- Sun Tao, He Hongbing. Research progress of platelet-rich fibrin in periodontal tissue regeneration. Journal of Oral Science Research. 2020; 36: 808-810.
- Chen Tielou, Liang XJ, Zhang XH. Do the fibrin scaffold and growth factors in platelet- rich fibrin play the most vital roles in bone re- generation. J Craniofac Surg. 2019; 30: 1923- 1926.
- He L, Lin Y, Hu X, Zhang Y, Wu H. A comparative study of Platelet- Rich Fibrin (PRF) and platelet-rich plasma (PRP) on the effect of proliferation and differentiation of rat osteoblasts in vitro. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009; 108: 707- 713.
- Duan XJ, Lin ZY, Lin XJ, Wang ZQ, Wu YH, et al. Study of platelet- rich fibrin combined with rat periodontal ligament stem cells in periodontal tissue regeneration. J Cell Mol Med. 2018; 22: 1047- 1055.
- Pradeep AR, Bajaj Pavan, Rao Nishanth S, et a1. Platelet-rich fibrin combined with a porous hydroxyapatite graft for the treatment of 3-wall intrabony defects in chronic periodontitis: A randomized controlled clinical trial. J Periodontol. 2017; 88: 1288- 1296.
- Castro AB, Meschi N, Temmerman A, et al. Regenerative potential of leucocyte- and platelet-rich fibrin. Part A: Intra-bony defects, furcation defects and periodontal plastic surgery. A systematic re- view and meta-analysis. J Clin Periodontol. 2017; 44: 67-82.
- Chen Tielou, Jiang Yifeng, Zhang Xinhai, Chen Jun, Huang Chuan- mei, et al. Morphological ultrastructure of platelet-rich fibrin and its implication. Journal of Tongji University (Medical Science). 2018; 39: 46-50.
- Nanditha S, Balamanikandasrinivasan C, Senthilkumar M, Kavitha M. Apprising the diverse facets of platelet rich fibrin in surgery through a systematic review. Int J Surg. 2017; 46: 186-194.
- Chen Tielou, Liu Jingchang, Liu Guoqin, Lin Shilong, Xu Heng, et al. Effects of hyperbaric oxygen on subgingival obligately, faculta-tively anaerobes and black pigmented bacteroides in periodontics pocket. J Pract Stomatol. 2010; 16: 75-78.
- Chen Tielou, Wang SF, Zhang XH, Chen J, Liu J. Synergistic Effects of Hyperbaric Oxygen Combining with Platelet Rich Plasma on Bone Defects Repair: A Mini-Review. J Dent & Oral Disord. 2020; 6(4): 1140.
- Awartani FA, Tatakis DN. Interdental papilla loss: Treatment by hy-aluronic acid gel injection: A case series. Clin Oral Investig. 2016; 20: 1775-1780.
- Aroca S, Keglevich T, Barbieri B, Gera I, Etienne D. Clinical evalu- ation of a modified coronally advanced flap alone or in combi- nation with a platelet-rich fibrin membrane for the treatment of adjacent multiple gingival recessions: A 6 month study. J Peri- odontol. 2009; 80: 244-252.
- Mustafa T, Hakan O, Taner A, Bahadir G, Levent P, et al. Clinical evaluation of autologous platelet-rich fibrin in the treatment of multiple adjacent gingival recession defects: A 12-month study. Int J Periodontics Restorative Dent. 2015; 35: 105-114.
- Chen Tielou, Lu HJ, Liu GQ, Tang DH, Zhang XH, et al. Effect of au- tologous platelet-rich plasma in combination with bovine porous bone mineral and biogide membrane on bone regeneration in mandible bicortical bony defects. J Craniofac Surg. 2014; 25: 215- 223.
- Wang Z, Feng Z, Wu G, Bai SZ, Dong Y, et al. The use of platelet-rich fibrin combined with periodontal ligament and jaw bone mesen- chymal stem cell sheets for periodontal tissue engineering.Sci Rep. 2016; 6: 28126.
- Chen Tie-lou, Zhang Xin-hai, Qin Wei-min, Wang Xiao-man, et al. Effects of calcined natural bovine bone combined with basic fi- broblast growth factor on periodontal intrabony defects. Chinese Journal of Practical Stomatology. 2018; 11: 224-228.
- Sharma A, Pradeep AR. Treatment of 3-Wall intrabony defects in patients with chronic periodontitis with autologous platelet-rich fibrin: A randomized controlled clinical trial. J Periodontol. 2011; 82: 1705-17l2.
- Johannes S, Pascal J, Martin S, Laurentiu B, Monika H, et al. Synergistic effects of HBO and PRP improve bone regeneration with autologous bone grafting. Injury. 2016; 47: 2718-2725.
- Gardin C, Bosco G, Ferroni L, Quartesan S, Rizzato A, et al. Hyperbaric oxygen therapy improves the osteogenic and vasculogenic properties of mesenchymal stem cells in the presence of inflam-mation in vitro. Int J Mol Sci. 2020; 21: 1452.
- Rocha FS, Gomes Moura CC, Rocha Rodrigues DB, Zanetta- Barbo-sa D, Nakamura Hiraki KR, et al. Influence of hyperbaric oxygen on the initial stages of bone healing. Oral Surg Oral Med Oral Pathol Oral Radiol. 2015; 120: 581-587.
- Izumino J, Kaku M, Yamamoto T, Yashima Y, Kagawa H, et al. Effects of hyperbaric oxygen treatment on calvarial bone regenera-tion in young and adult mice. Arch Oral Biol. 2020; 117: 104828.
- Fok TC, Jan A, PeelL SA, Evans AW, Clokie CML, et al. Hyperbaric oxygen results in increased Vascular Endothelial Growth Factor (VEGF) protein expression in rabbit calvarial critical-sized defects. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008; 105: 417-422.
- Sunkari VG, Lind F, Botusan IR, Kashif A, Liu ZJ, et al. Hyperbaric oxygen therapy activates hypoxia-inducible factor 1 (HIF-1), which contributes to improved wound healing in diabetic mice. Wound Repair Regen. 2015; 23: 98-103.
- Yuce HB, Gokturk O, Turkal HA, Inanir A, Benli I, et al. Assessment of local and systemic 25-hydroxy-vitamin D, RANKL, OPG, and TNF levels in patients with rheumatoid arthritis and periodontitis. J Oral Sci. 2017; 59: 397-404.