SciBase Journals
SciBase Dentistry and Oral Sciences
- Article Type: Research Article
- Volume 2, Issue 2
- Received: Sep 04, 2024
- Accepted: Oct 17, 2024
- Published Online: Oct 24, 2024
The Evaluation of the Diagnostic Value of Mean Platelet Volume in Isolated Mandible Fractures
Hamdi Sari1; Müge Çina2*; Nesrin Gökben Beceren3
1Private Practice, Deutsche Approbation BW, Freiburg, Deutschland, Germany
2Assoc. Prof. Dr. Suleyman Demırel University, Faculty of Dentistry, Department of Oral and Maxillofacial Surgery, Isparta, Turkey.
3Prof. Dr. Suleyman Demırel University, Faculty of Medicine, Department of Emergency Medicine, Isparta, Turkey.
*Corresponding Author: Müge Çina
Suleyman Demirel University, Faculty of Dentistry, Department of Oral and Maxillofacial Surgery, Isparta, Turkey.
Tel: +905324713066;
Email: mugecina@hotmail.com
Abstract
Objective: Mandibular fractures, a type of maxillofacial trauma, are commonly seen in emergency services. In this retrospective study, we aimed to determine the mean platelet volume (MPV) value and to investigate the diagnostic value of isolated lower jaw fractures in predicting the prognosis according to the location of the fracture in the jaw.
Materials and methods: 50 patients were found suitable for eligibility criteria as a study group and 44 healthy individuals were included in the control group. Age, sex, white blood cell (WBC), and MPV values were compared between groups.
Results: The mean MPV value of study group (7.864±0.129) was found to be lower than control group’s (8.476±0.161). Mean WBC value of study group (12.530±0.653) was found to be higher than that of the control group (7.360±0.297). Mean WBC and MPV levels were found to be significantly different between groups (p< 0.01).
Conclusions: Although MPV and WBC levels were not significantly different in isolated fracture localizations of the mandible, both MPV and WBC levels were seen at higher levels in patients with multiple fracture sites than in patients with one fractured site.
Keywords: Emergency service; Trauma; Mandible; Fracture; Mean platelet volume.
Citation: Sari H, Çina M, Gökben Beceren N. The Evaluation of the Diagnostic Value of Mean Platelet Volume in Isolated Mandible Fractures. SciBase Dent Oral Sci. 2024; 2(2): 1016.
Introduction
Trauma is the most common cause of death [1]. Maxillofacial trauma as a subtype of trauma is often encountered in emergency services. Although some of these patients have other region fractures or blunt traumas simultaneously with maxillofacial trauma, some of them have only maxillofacial fractures [2,3] Patients with maxillofacial trauma are 45.3-60% of all trauma patients [3-5]. In maxillofacial traumas, the mandible is the most often fractured bone. Due to the mandible’s location with respect to the rest of the skull and relative prominence compared to the other facial bones, it is more easily fractured [6]. Mandible fractures are found to be between 45.4 and 75% of all maxillofacial region fractures [7,8]. In mandible fractures, as with other bone fractures, there are some factors affecting the prognosis, such as the fracture type, the displacement of fragments, the localization of the fracture, the type of trauma (blunt or sharp), the vector and severity of impact. We must consider all these factors for the prognosis. Trauma initiates a multifaceted cascade reaction consisting of hemodynamic, metabolic, neuroendocrine and immune processes [9]. For these patients’ treatment planning and prognosis, it is important to ensure a detailed examination and further investigation (as with biochemistry and radiology). In nearly all trauma patients, when they are admitted to the emergency department, a biochemical analysis (a complete blood count and enzyme tests) is done in addition to physical and radiological examination. In a complete blood count, the white blood cell (WBC), platelet, lymphocyte, hemoglobin, hematocrit, Mean Platelet Volume (MPV) levels, and other blood parameters are all assessed. Platelet and WBC counts are the markers that show the inflammatory reaction [10]. In previous studies, MPV was found to have a coordination role in proinflammatory and prothrombotic processes (in which inflammatory cytokines like IL-1, IL-6, TNF-α, and thrombopoietin regulate thrombopoiesis). MPV is also linked to platelet function and activation, and platelet size within blood circulation is an evident marker for evaluating the severity of systemic inflammation [11]. Yolcu et al. found a relation between MPV, the WBC levels of trauma patients and the severity of trauma. They suggested that MPV is a helpful marker for predicting the severity of trauma [12]. In this study, we aimed to investigate the prognostic value of MPV in trauma patients who had isolated mandible fractures.
Materials and methods
Ethics committee approval: This retrospective study was performed with permission from the Suleyman Demirel University Clinical Trials Ethics Committee (17.12.2014/216). The study was carried out following the international declaration of Helsinki.
Study setting: Fifty trauma patients with isolated mandible fractures were included in this study. All of the patients had been admitted to Suleyman Demirel University Medical Faculty Emergency Services for five years. A control group of 44 healthy adults were investigated retrospectively as a study group from the database, and included in this study. Age, gender, initial laboratory findings, fracture localizations in the mandible, and the displacement of fragments in mandible fractures were investigated.
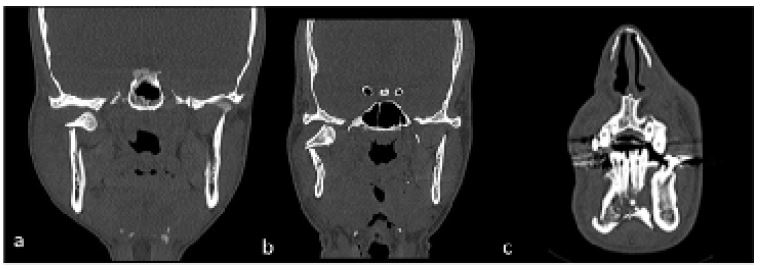
We found 186 trauma patients from the database who had mandible fractures in their initial diagnosis. We accessed these patients’ information, and we examined laboratory measures and computerized tomography images at all sections (axial, coronal and sagittal) (Figure 1).
We found 50 patients who had isolated mandible fractures and were suitable for our eligibility criteria. The eligibility criteria of the study were: to be older than 18 years old, to have no other bone fractures except the mandible and as well as to have no history of chronic inflammatory diseases, cardiometabolic diseases, or stroke. Exclusion criteria of the study were: to be younger than 18 years old, have a history of a disease that may affect MPV value, such as chronic inflammatory diseases, not to have radiographical images or a complete blood count, and not to have any other body region fractures besides the mandible. In the control group, we found 44 healthy people retrospectively from the database. We investigated age, gender and mandible fracture localization based on Natvig and Dingman’s classification [13]. We compared the WBC and MPV levels of the trauma patients with those of the healthy control groups.
Statistical analysis: In this study, the SPSS 18.0 program was used for statistical analysis. Continuous variables such as blood parameters, MPV, and WBC were analyzed using the ANOVA factorial variance analysis technique. Group factors had two variables (trauma group and control group), and gender factors had two variables (male and female). Localization and displacements were also investigated by variance analysis technique with gender feature together separately. Differences in the means of the groups were compared by Tukey, which is one of the multiple comparison tests.
Results
Fifty patients with isolated mandible fractures were included in this study; these were 42 males (84%) and 8 females (16%). Forty-four healthy people, 24 males (54.54%) and 20 females (45.45%), were included in the control group. The total of the study and control groups was 66 males (70.21%) and 28 females (29.78%). The mean ages of the study group and the control group were 34.28±2.37 and 58.2±1.52, respectively. The difference in mean age values between groups was statistically significant (p< 0.01). We found that the study group was younger than the control group (Table 1).
Table 1: Group and gender distribution mean values for age.
| Age | Female (n=28) | Male (n=66) | Total (n=94) |
|---|---|---|---|
| Study group,(n=50), Mean±SD | 38.63 ±8.38 (16%) | 33.45±2.36 (84%) | 34.28±2.37b |
| Control group, (n=44), Mean±SD | 61.75±2.17 (45.45%) | 55.25±1.97 (54.54%) | 58.2±1.52a |
| Total, Mean±SD | 55.14±3.41 (29.28%) | 41.38±2.10 (70.21%) |
a and b: Statistical differences are indicated with letters, statistically significant differences between the groups are stated with different letters (p ˂0.01); SD: Standard deviation.
The mean MPV values in the study and control groups were 7.864±0.129 and 8.476±0.161, respectively. MPV levels were significantly different between groups (p< 0.01). We found that MPV levels in trauma patients were lower than those in the control group (Table 2).
Table 2: Group and gender distribution mean values for MPV.
| MPV | Female | Male | Total |
|---|---|---|---|
| Study group, Mean±SD | 7.625±0.313 | 7.910±0.142 | 7.864±0.129b |
| Control group, Mean±SD | 8.447±0.280 | 8.500±0.188 | 8.476±0.161a |
| Total, Mean±SD | 8.212±0.228 | 8.124±0.118 |
a and b: Statistical differences are indicated with letters, statistically significant differences between the groups are stated with different letters (p˂0.01); SD: Standard deviation.
Table 3: Group and gender distribution mean values for WBC.
| WBC | Female | Male | Total |
|---|---|---|---|
| Study Group, Mean±SD | 14,55±2,62 | 12.145±0.601 | 12.530±0.653a |
| Control Group, Mean±SD | 7.237±0.398 | 7.642±0.438 | 7.360±0.297b |
| Total, Mean±SD | 9.327±0.996 | 10.442±0.498 |
a and b: Statistical differences are indicated with letters, statistically significant differences between the groups are stated with different letters (p ˂0.01); WBC: White blood cell; SD: Standard deviation.
The mean WBC value in the study group was 12.530±0.653, whereas in the control group, the mean WBC value was 7.360±0.297. Mean WBC levels were significantly different between groups (p< 0.01). Levels of WBC in trauma patients were higher than those in the control group (Table 3).
When the blood parameters were investigated according to age, gender, localization of fractures, and fractures with displacement and the interactions between them, age was significantly different between all localizations (p< 0.05), but not between genders (p< 0.01). MPV and WBC levels were not found to be significantly different between genders (p< 0.01), fracture localizations (p< 0.05), or displaced and undisplaced fractures. When isolated mandible fracture localizations were investigated for age, gender and blood parameters, the mean age values between patients with isolated angulus and condyle fractures were significantly different. We found that patients with isolated angulus fractures were younger than patients with condyle fractures. There was no significant difference between other localizations for the variable of age. MPV and WBC levels were not found to be significantly different in isolated mandible fracture localizations (Table 4).
Table 4: The minimum-maximum and mean values of parameters (age, MPV, WBC) in isolated mandible fracture localizations.
| Fracture Localizations | AGE | MPV | WBC | |||
|---|---|---|---|---|---|---|
| Min-Max | Mean±SD | Min-Max | Mean±SD | Min-Max | Mean±SD | |
| Isolated Symphysis Fractured Patients, (n=3) | 27-50 | 37.33±6.74ab | 6.1-7.9 | 7.167±0.546 | 6.7-20.1 | 13.9±3.9 |
| Isolated Corpus Fractured Patients, (n=14) | 21-82 | 39.0±4.95ab | 7.2-9.4 | 8.007±0.162 | 6.4-23.3 | 12.5±1.23 |
| Patients with corpus. condyle and ramus fractures, (n=3) | 22-33 | 26.67±3.28ab | 7.3-10.3 | 8.367±0.968 | 11.8-15.6 | 14.33±1.27 |
| Isolated Angulus Fractured Patients, (n=13) | 18-43 | 25.62±1.9b | 6.6-8.6 | 7.577±0.191 | 4.8-17.2 | 12.28±1.06 |
| Isolated Ramus Fractured Patients, (n=6) | 18-57 | 30.17±5.59ab | 6-9.3 | 7.55±0.492 | 6.5-27 | 14.1±3.03 |
| Isolated Condyle Fractured Patıents, (n=9) | 20-78 | 45.78±7.8a | 7.1-10 | 8.222±0.366 | 4.1-16.5 | 10.0±1.14 |
a and b: Statistical differences are indicated with letters, statistically significant differences between the groups are stated with different letters (p ˂0.01), SD: Standard deviation; WBC: White blood cell; MPV: Mean platelet volume
Discussion and conclusion
Maxillofacial traumas, as a subtype of general trauma, have a significant proportion of these, and mandible fractures are one of the most common fractures in the maxillofacial region. Kırış et al. found that 64.6% of all maxillofacial fractures are mandible fractures [14], and Erol et al. found 2111 patients with isolated mandible fractures out of 2901 patients have maxillofacial fractures [7]. Considering the mandible’s prominent position in the face, these findings are not surprising at all.
MPV is often overlooked in complete blood count but is gaining importance among physicians. It has been found to be associated with platelet activation and function. Higher MPV levels are accepted as an independent risk factor for coronary artery and cerebrovascular diseases. There is a consensus that platelet volume is determined during the production of platelets from megakaryocytes. Generally, when the platelet count decreases, the MPV level increases. More giant platelets are considered to be younger and more active compared to smaller platelets. It is believed that more giant platelets secrete more β-thromboglobulin and thromboxane A2 [15,16]. MPV value alterations have prognostic value in terms of the thrombotic and prothrombotic processes. MPV has varying values for many diseases. Yolcu et al. found that MPV, WBC, and platelet levels were significantly different in trauma patients, and they suggested that MPV might be an inflammatory marker in trauma patients [7]. Jacoby et al. found a direct proportion between the severity of trauma and an increase in platelet function and activation in their study [17]. Relation between trauma-metabolic response and mortality is well known today. After trauma, the body response starts at the cellular level, and this causes tachycardia, catabolism, and elevated body temperature. The body’s energy and oxygen consumption increase in relation to the severity of trauma [18]. Platelet and WBC counts are important markers in the first steps of the post-traumatic process. Platelet contraction is clinically relevant because it demonstrates platelet hyperactivity in trauma survivors and dysfunction in nonsurvivors [19]. In our study, MPV levels in the study group were found to be lower than the control group. Yolcu et al. investigated the severity of trauma with an initial Glasgow Coma Scale (GCS) and Revised Trauma Scores (RTS), and they reported that the severity of trauma is significantly related to GCS and RTS [12].One possible explanation is that our study group included isolated mandibular fractures, and a trauma that resulted in only a mandibular fracture might not be as severe as that which produced life-threatening conditions (as in general trauma). The body’s response to trauma changes as the severity of inflammation decreases, so blood parameters might not change at those levels in the same way as in general traumas. WBC levels were found to be higher in our study group. Post-traumatic leukocytosis was verified in many studies. Rovlias et al. studied 624 patients with severe injury and reported that in severe head injury patients, WBC counts were significantly higher than in minor or moderate injury patients [20]. Akköse et al. reported a significant relation between the severity score of an injury and blood leukocyte levels [21]. The results of the presented study showed that MPV and WBC levels did not significantly alter in response to isolated fractures localized in the mandible. Although they were not significantly different, both MPV and WBC levels were found at higher levels in the three patients with multiple fracture sites than in patients with only one fracture site. This might be because a trauma that was capable of fracturing multiple localizations in the mandible was more significant than the force of a trauma that merely caused a fracture in one localization, so the increased severity of trauma might have affected MPV and WBC levels in the blood.
In conclusion, patients with mandible fractures are often encountered in emergency services. Isolated mandible fracture starts an inflammatory process, as with all traumas. The WBC level changes in the post-traumatic process are well known. We researched MPV levels in patients with isolated mandible fractures, and according to our results, we may say that MPV may not have the diagnostic value of isolated mandible fractures which occurred in one localization in the mandible. However, in our study, even though the result is not statistically significant, patients with multiple fractured mandible localizations have higher MPV levels. Further comprehensive prospective trials are needed to determine the value of MPV levels for predicting the prognosis of maxillofacial fractures.
Declarations
Ethics committee approval: Our study was approved by the Suleyman Demirel University Clinical Trials Ethics Committee (17.12.2014/216). The study was carried out following the international declaration, guidelines.
Conflict of interest: No conflict of interest was declared by the authors.
Author contributions: Concept - MC, HS; Supervision - MC, NGB; Materials - HS, MC, NGB; Data Collection and/or Processing - HS, MC; Analysis and/or Interpretation - MC, HS; Writing -HS, MC.
Other information: Our study was produced from a Specialization Thesis (Number: 454122) and presented at AÇBİD 10th International Congress as an oral presentation.
References
- Kim JK, Sun KH. Role of platelet-to-lymphocyte ratio at the time of arrival to the emergency room as a predictor of short-term mortality in trauma patients with severe trauma team activation. Acute Crit Care. 2024; 39(1): 146-154.
- Yüksel A, Sabri U. Maxillofacial trauma. Türkiye Klinikleri J Surg Med Sci. 2006; 2(28): 59-67.
- Gassner R, Tuli T, Hächl O, Rudisch A, Ulmer H. Cranio-maxillofacial trauma: a 10 year review of 9543 cases with 21067 injuries. J Craniomaxillofac Surg. 2003; 31(1): 51-61.
- Kamulegeya A, Lakor F, Kabenge K. Oral maxillofacial fractures seen at a Ugandan tertiary hospital: a six-month prospective study. Clinics. 2009; 64(9): 843-848.
- Wanderley da SF, Fanderuff M, Reis TVR, Rebellato NLB, Scariot R, Klüppel LE. Atypical Mandibular Angle Fracture. J Craniofac Surg. 2019; 30(2): 155-157.
- Chukwulebe S, Hogrefe C. The Diagnosis and Management of Facial Bone Fractures. Emerg Med Clin North Am. 2019; 37(1): 137-151.
- Erol B, Tanrikulu R, Görgün B. Maxillofacial Fractures: Analysis of demographic distribution and treatment in 2901patients (25-year experience). J Cranio-Maxillofac Surg. 2004; 32(5): 308-313.
- Wusiman P, Maimaitituerxun B, Guli Saimaiti A, Moming A. Epidemiology and Pattern of Oral and Maxillofacial Trauma. J Craniofac Surg. 2020; 31(5): 517-520.
- Pape HC, Moore EE, McKinley T, Sauaia A. Pathophysiology in patients with polytrauma. Injury. 2022; 53(7): 2400-2412.
- Sandhaus LM, Meyer P. How useful are CBC and reticulocyte reports to clinicians? Am J Clin Pathol. 2002; 118(5): 787-793.
- Yuri Gasparyan A, Ayvazyan L, P Mikhailidis D, D Kitas G. Mean platelet volume: a link between thrombosis and inflammation? Curr Pharm Des. 2011; 17(1): 47-58.
- Yolcu S, Beceren GN, Tomruk Ö, Doğuç DK, Balbaloglu O. Can mean platelet volume levels of trauma patients predict severity of trauma? Platelets. 2014; 25(4): 279-284.
- Owusu JA, Bellile E, Moyer JS, Sidman JD. Patterns of Pediatric Mandible Fractures in the United States. JAMA Facial Plast Surg. 2016; 18(1): 37-41.
- Kırış M, Köksal Y, Çelebi S, Kıroğlu F, Çankaya H. Maksillofasiyal kırıklarda tedavi yaklaşımımız: Retrospektif inceleme. Türkiye Klinikleri J Surg Med Sci. 2009; 29(3): 696-701.
- Bath P, Algert C, Chapman N, Neal B. Association of mean platelet volume with risk of stroke among 3134 individuals with history of cerebrovascular disease. J Cerebral Circul. 2004; 35(3): 622-626.
- Rustiasari UJ, Roelofs JJ. The Role of Platelets in Diabetic Kidney Disease. Int J Mol Sci. 2022; 23(15): 8270.
- Jacoby RC, Owings JT, Holmes J, Battistella FD, Gosselin RC, Paglieroni TG. Platelet activation and function after trauma. J Trauma. 2001; 51(4): 639-647.
- Corbett SA. Systemic Response to Injury and Metabolic Support. In: Brunicardi F, Andersen DK, Billiar TR, Dunn DL, Kao LS, Hunter JG, Matthews JB, Pollock RE. eds. Schwartz’s Principles of Surgery, 11e. McGraw-Hill Education. 2019.
- George MJ, Aroom KR, Wade CE, Cox CS, Gil, BS. A Novel Platelet Function Assay for Trauma. J Surg Res. 2020; 246: 605-613.
- Rovlias A, Kotsou S. The blood leukocyte count and its prognostic significance in severe head injury. Surg Neurol. 2001; 55(4): 190-196.
- Akköse S, Bulut M, Armağan E, Balcı V, Yolgösteren A, Ozgüç H. Does the leukocyte count correlate with the severity of injury? Ulus Travma Acil Cerrahi Derg. 2003; 9(2): 111-113.