SciBase Journals
SciBase Epidemiology and Public Health
ISSN 2691-7785
- Article Type: Research Article
- Volume 1, Issue 1
- Received: Oct 10, 2023
- Accepted: Dec 01, 2023
- Published Online: Dec 07, 2023
Impact of COVID-19 Pandemic on University Students of Bangladesh: A Cross-Sectional Study
Faruq Mohammad O1*; Habib Samira H2; Mahjabeen M3
1Am. Board Cert Int. Med. Professor and Chief Consultant, United Medical College and United Hospital Ltd, Gulshan, Dhaka 1212, Bangladesh.
2Principal Research Officer and Associate Professor, Health Economics Unit, Diabetic Association of Bangladesh, Dhaka 1000, Bangladesh
3Intern, Shaheed Suharawardy Medical College, Dhaka, Bangladesh.
*Corresponding Author: Faruq Mohammad O
Am. Board Cert Int. Med. Professor and Chief Consultant, United Medical College and United Hospital Ltd, Gulshan, Dhaka 1212, Bangladesh.
Tel: +8801674999897
Email: faruqmo@yahoo.com
Abstract
Background: During the COVID-19 pandemic of 2019-20 university students of Bangladesh like many other countries suffered from impact of this pandemic in terms of education, general health and wellbeing.
Methods: A ‘low risk’ questionnaire with modified General Health (GHQ-28) and General Anxiety Disorder (GAD-7) instruments were shared with university students of Bangladesh via an email link over 4-weeks as a part of a larger international study involving several countries.
Results: 145 Bangladeshi university students responded. Most of respondents came from capital city of Dhaka. Age varied between 15 and 22 years and male female ratio was 65:35. First year students comprised 28%. 78% students used on line education only. 73 % students claimed that the quality of education during pandemic was poor. 60% found it difficult to adapt to new teaching methods like (Zoom class, online class). 37% students faced general health difficulties and 5% suffered from severe general anxiety disorder.
Conclusion: Universities should modify the virtual training methods and enhance the mental health and wellbeing support before disaster like COVID pandemic strikes again.
Citation: Faruq MO, Habib SH, Mahjabeen M. Impact of COVID-19 Pandemic on University Students of Bangladesh: A Cross-Sectional Study. SciBase Epidemiol Public Health. 2023; 1(1): 1005.
Introduction
The COVID -19 virus was first identified in Wuhan, China, in December 2019 [1]. On March 11, 2020, the World Health Organization declared the infection a pandemic [2] and the first three cases of COVID-19 were found in Dhaka, Bangladesh on March 08, 2020 [3]. Given the dense population of Bangladesh and other factors, COVID-19 became a major public health concern in Bangladesh, as in other countries. In Bangladesh like in many other countries pandemic situation hindered university students’ studies, disrupt their daily routines [4] and habits, and had an impact on their mental health. Further, home quarantine, physical/spatial distancing, and other restrictions were likely to have psychological impacts on students [5] and negatively influenced their mental wellbeing [6].
While quarantined and out of the university environment and schedule, students might experience stress, anxiety, anger, boredom, loneliness, and other emotions, with both shorterand longer-term impacts [7,8]. In the shorter-term, such feelings may lead to sleep problems, changes in eating habits, and engagement in potentially addictive behaviors, and some of these factors may then also increase depression, anxiety, and stress [9]. News, misinformation, and rumors about COVID-19 might also increase negative thoughts and emotions [10] within students and about their futures. A prior off line study reported high levels of moderate to extremely severe depression (52.2%), anxiety (58.1%), and stress (24.9%) during pre-COVID-19 periods among university students in Bangladesh [11]. Several factors leading to depression, anxiety and stress among students have been established in existing literature, including sex, strained relationships, family and peer pressure, lack of financial support and hardship, high parental expectations, sleep deprivation, problematic internet use, isolation, toxic psychological environment, academic pressure, workload, and heavy test schedules [12-16].
Approximately 1.5 billion students worldwide were affected due to educational institution closures [17]. According to learning lab Bangladesh COVID-19 Multi-sector impact report, almost 60 percent of the students have not even heard from institutions about how the educational activities will continue. According to 38 percent of parents, there was no continuity in teaching [18]. Household income expenditure survey claimed that 8.4 million student’s families across the world live below the poverty level. Their income has dropped by 25% in the first three months of COVID pandemic [19]. It was observed that COVID-19 had a driven, devastating impact on low-income countries like Bangladesh. As a result, so it was often impossible for most students of Bangladesh to get online education through expensive devices. Most teachers did not have high-cost internet devices because their monthly income rate was low.
The aim of our study was 1) To estimate the volume of impact of COVID-19 on students of universities of Bangladesh regarding educational, financial and psychological issues and 2) To explore the availability and accessibility of internet and devices for online class for the students of universities to overcome the impact and challenges.
Materials and methods
Our study was Bangladesh part of an international study entitled “A students perspective on university education and wellbeing one year into the COVID -19 pandemic” [20]. It was participated by university students from England, South Africa, Sri Lanka, Pakistan besides Bangladesh. Our study, which was done in Bangladesh was cross-sectional and study design was analytical in nature. A cohort of 145 students responded from Bangladeshi universities during the month of November and early December 2020. Students from public, private, and national universities in Bangladesh participated in the survey from eight divisional regions. The questionnaire of the above-mentioned study was taken as an established and validated questionnaire for our study. The survey was conducted with an online survey tool (Google Forms). A Google link of the questionnaire was circulated among the participants recruited purposively through e-mail of personal communication and an online survey. The answer format of the questionnaire was auto saved and documented in the drive of the analytical sheet.
No incentives or rewards were offered for participation. During the survey, individuals first provided informed consent and then were asked the questions. The inclusion criteria to participate in the study were being a Bangladeshi university student, having internet access, being willing to respond voluntarily and submit a completed survey. The exclusion criteria was non consent.
Ethical approval was granted by the King’s College London (UK) Research Ethics Committee [20]. The letter of UK ethical approval was dispatched to all collaborating countries including Bangladesh to enable them to acquire local ethical clearances. Participants were contacted by email, via the relevant institution of their learning. Participation was voluntary and anonymous. The survey data were collected anonymously, and all participants gave their written informed consent to participate. The consent form clearly documented the (i) nature and procedure of the study, (ii) aims of the study, (iii) anonymity and confidentiality of data, (iv) choice to participate in the study, and (v) right to revoke data at any time from the study.
Novel set of questions were used to explore the impact COVID-19 had on student life, and its impact on education. Open ended questions explored the subjective experiences of students and their aspirations for the future. The survey included both multiple-choice and open questions which took an estimated 20 minutes to answer. The questionnaire was subcategorized into five domains. Quantitative data were collected from Domain 1 to 5.
Domain 1 - The information letter, consent, and demographics. This included the participant invitation letter, consent form, a request for a fake ID and questions on demographics.
Domain 2 - Impact of COVID-19 on University Life. This section of the questionnaire explored how COVID-19 had affected students, socially and financially and the different challenges they were facing.
Domain 3 - Impact of COVID-19 on University Education. This section gathered the students’ opinions on both the positive and negative aspects of new modes of ‘virtual’ learning and possible improvements.
Domain 4 - Impact of COVID-19 on General Health Questionnaire (GHQ). General Health questionnaire GHQ-28 [21] a validated instrument was used to assess public health.
The GHQ-28 questionnaire consisted of four sub-components that measured public health (somatic symptoms, anxiety and insomnia, social dysfunction, and depression), and each component consisted of 7 questions. GHQ scoring methods were based on the Likert scale from zero to three and a lower score indicates a better mental state. The scoring system applied in this study was the same as the original scoring system, the Likert scale 0,1,2,3. The minimum score for the 28 version is 0, and the maximum is 84. Higher GHQ-28 scores indicated higher levels of distress. GHQ-28 was a multiple-choice, self-administered, validated instrument. However, the last 5 questions of GHQ-28 explored suicidal intent and were modified here to explore ‘intent to leave university’. With the modifications, the instrument qualified as a ‘low risk’ instrument for participant. This modified GHQ-28, was named GHQ-28(M) [20].
Domain 5 - Impact of COVID-19 on mental health. We used Generalized Anxiety Disorder GAD-7 [22], a validated instrument to assess general anxiety disorder states. The GAD-7 score was calculated by assigning scores of 0,1,2, and 3, to the response categories of “not at all,” “several days,” “more than half the days,” and “nearly every day,” respectively, and then adding together the scores for the seven questions. GAD-7 total score for the seven items ranges from 0 to 21. The GAD-7 represents an anxiety measured based on seven items, which were scored from zero to three. The final question of the GAD-7 was removed to maintain the ‘low risk’ status of the questionnaire for this study. GAD-7 scores 0-21, and identified >10 as moderate and >15 as severe anxiety disorder. Our modified score, now named GAD-6 [20], scored 0-18 and was proportionately adjusted to identify the severity of anxiety. For GHQ-28M and GAD-6 median (range) were used to interpret the results.
Thematic analysis: The data for the qualitative analysis was extracted from the comments and suggestions provided by participants in Domain 2 and 3 on the open questions. These questions explored the positive and negative aspects of new ‘virtual’ modes of study, the impact of online exams, and areas participants felt could be improved with suggestions to achieve this. This process was termed as thematic analysis (see results section on thematic analysis and Table 3).
Statistical analysis on quantitative data: Data analysis was performed using Microsoft Excel 2019 and IBM Statistical Package for Social Scientists (SPSS) Statistics version 20.0. Microsoft Excel was used for editing, sorting, and coding. Next, the excel file was imported into SPSS software. Descriptive statistics (frequencies, percentages) were executed using SPSS software. Relevant data were expressed through table and graphical presentation. All tests were 2-tailed, and P<0.05 was considered statistically significant. Continuous data were described and analyzed based on their distribution, be it parametric or nonparametric. Outcomes were compared across groups, where appropriate, using Mann-Whitney/Wilcoxon test or student t-test for continuous data or the chi square χ2 or the Fisher’s exact test for categorical data. A univariate analysis was used to identify possible associations of demographics with outcomes.
Table 1: Age varied from 15 to 22 Yrs.
| Variables | Description | Percentage |
|---|---|---|
| Division | ||
| Dhaka | 44(30.34) | |
| Rajshahi | 19(13.10) | |
| Chittagong | 23(15.86) | |
| Khulna | 17(11.72) | |
| Barishal | 15(10.34) | |
| Sylhet | 13(8.96) | |
| Mymensingh | 9(6.20) | |
| Rangpur | 5(3.44) | |
| Sex | ||
| Male | 94 (64.8) | |
| Female | 51 (35.2) | |
| Age | ||
| 15-16 | 5 (3.4) | |
| 16-19 | 87(60.0) | |
| 19-22 | 53(36.6) |
Table 2: The impact of courses pattern during pandemic period.
| Course changes during pandemic | ||
|---|---|---|
| Changes | Number | Percentage |
| Completely | 18 | 12 |
| Not at all | 41 | 28 |
| Quite a lot | 37 | 26 |
| Some variation | 49 | 34 |
| Total | 145 | 100 |
| Interaction of classes during pandemic period | ||
| Neutral | 62 | 42.8 |
| No | 49 | 33.8 |
| Yes | 28 | 19.3 |
| Total | 145 | 100.0 |
| Education comparison before and after pandemic | ||
| Better | 18 | 6.2 |
| Poor | 106 | 73.1 |
| Same | 21 | 14.5 |
| Total | 145 | 100.0 |
| University support during COVID period | ||
| I don't know | 12 | 8.3 |
| Neutral | 44 | 30.3 |
| No | 52 | 35.9 |
| Not that much | 1 | .7 |
| Yes | 36 | 24.8 |
| Total | 145 | 100.0 |
| Frequently monitoring the course materials and resources | ||
| Didn’t response | 35 | 24.1 |
| Never | 43 | 29.7 |
| Occasionally | 40 | 27.6 |
| Often | 2 | 1.4 |
| Sometimes | 25 | 17.2 |
| Total | 145 | 100.0 |
| Examination should hold during pandemic time | ||
| Didn’t response | 20 | 13.8 |
| No | 52 | 35.9 |
| Yes | 73 | 50.3 |
| Total | 145 | 100.0 |
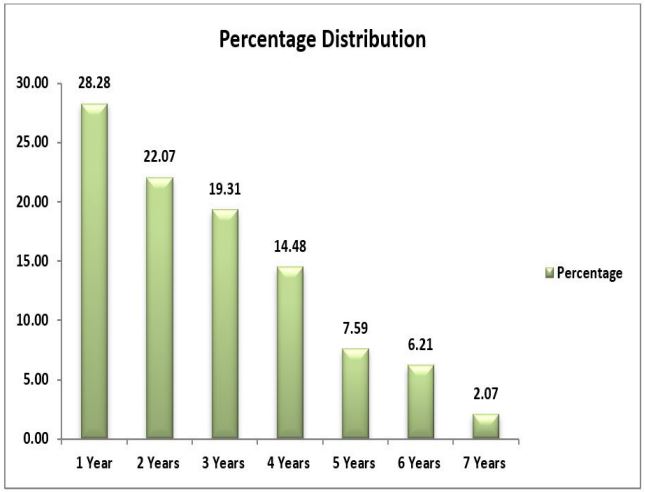
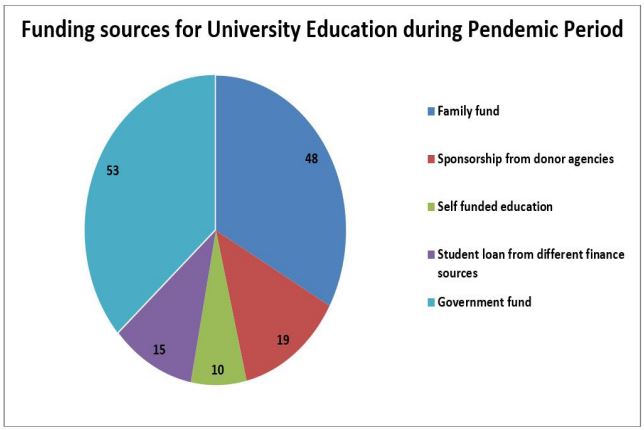
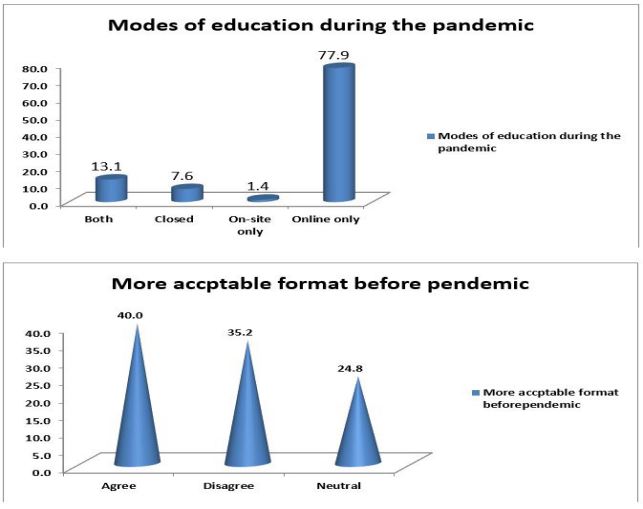
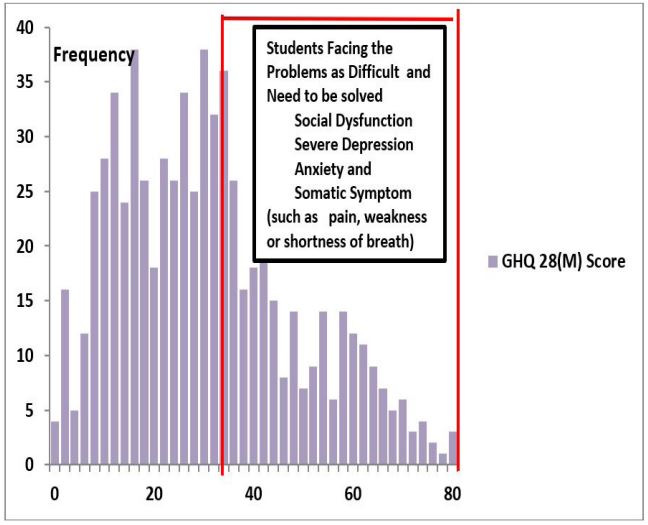
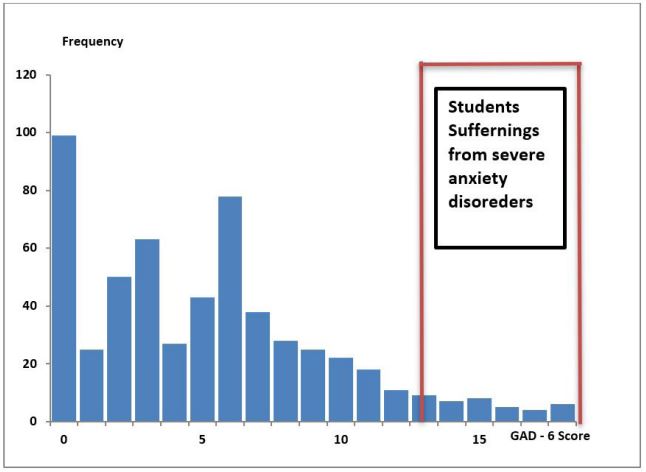
Table 3: Thematic Idea about virtual teaching.
| Positive aspects |
• Increased quality of
learning due to internet
access and cope with the new
modules • Increased quality time with family • Health and mental well-being due to safe stay at home |
|---|---|
| Difficulties faced |
• Digital unavailability due
to low middle income of the
society as a whole (costs of
software, hardware, con- nectivity of WiFi) • Students and teachers not conversant with online learning • Scheduled examinations postponed |
| Negative attitudes |
• Poor interaction with
lecturers and peers • Poor learning efficacy • Increased screen time leading to lethargy |
|
Why students accessed
additional re- sources in parallel |
• Inconvenient and
insufficient lectures and
materials provided through
online • To support future careers and skill development • Poor access to journals or textbooks from library |
| Assessments |
• Disparity between teaching
and assessment • Feeling more fatigue and lethargic during class lecture • Increased risk of cheating |
| How to improve online learning |
• Ensure library resources
are more easily
accessible • Provision of improved software interface for easier access • Open dialogue between students and academic staff |
| How to improve online examinations |
• Accessibility of user
friendly software • Technique obtained to reduce cheating • format of exams should be clear cut |
| Post-pandemic continuations |
• Continuing online
examinations and
assessment • Record lectures and make them available for revision |
| Cost-benefit or lack thereof |
• Financial challenges
confronting students and
their families • Academic staff have embraced the move to distance learning |
| How can we improve distance learning |
• Induction sessions for
students to access digital
resources • Increase engagement between academic staff and students for example, live sessions for questions • Effective use of available technology |
Results
A) Impact on socio demographic status (Domain 1 and 2): A total of 145 student responded to the study. They were from different districts of eight divisional part of Bangladesh. Most of the study subjects are from capital city Dhaka (30.34%). Male comprised 64.8% and female comprised 35.2% of the participants. They were from various academic disciplines like Science, Commerce and Humanities background with different academic years. Their age varied from 15 to 22 Yrs (Table 1). Figure 1 shows percentage distribution of students by academic year of study. There were comprehensible variations in the way the students funded their university education. The analysis found that there were accommodation as ‘private’ (own home, parent’s home, and commuting) and ‘shared’ (university halls, boarding houses, and rented accommodation with shared facilities). During the pandemic period, the students shifted towards private accommodation frequently. When we collected data on funding sources of their education, we found that there were various funding sources like family fund, sponsorship from donor agencies, self-funded education, student loan from different finance sources, government fund etc (Figure 2).
B) Impact on student education (Domain 3): A bulk of students (51.7%), stated that the quality of education level they were receiving during pandemic period were lower compared to prior to the pandemic. A majority (59.7%) of students found it difficult to adapt to new teaching methods (zoom classes, online course, online assignment submission and so on) and 37% felt stressed at levels higher than pre pandemic period. Additionally, 42.4% of participants did not have an allocated personal tutor, and of those that did, 7.2% did not feel supported by their personal tutor. Most of the pending exams were held during pandemic time (73.9%). Those exam formats were mainly ‘written remote computer based’ or ‘remote viva, via the internet’. Students found these exams were more stressful compared to previous examination formats. Moreover, 49.5% of students expressed concern over post-pandemic job opportunities. Table 2 showed the impact of courses pattern during pandemic period. Figure 3 and 4 showed modes of education and acceptable format of education system during pandemic period respectively.
C) Impact on general health and mental health status of the students (Domain 4 and 5): GHQ-28(M) (n=145) and GAD6 (n=145) scores (n=145) scores were not normally distributed (Shapiro-Wilk test p<0.005). Frequency distribution curves of GHQ-28(M) and GAD-6 were drawn to understand the prevalence of disturbed physical and mental health situations among students. The median (range) GHQ-28(M) and GAD-6 scores were 31.0 (0-77) and 7.0 (0-18) respectively. In a univariate analysis, neither the GHQ-28(M) scores nor the GAD-6 scores were significantly associated with age group, gender, year of study or various pattern of education module delivery. The total group was analyzed using a non-parametric approach and not by regression analysis. Frequency distribution of the GHQ-28(M) and GAD-6 total score was observed to be skewed compared to the normal distribution (Figures 5 and 6). At the zero end of the distribution, there was a greater skewness and greater departure between the mean and median values. This implied that the mean value might be sensitive to the skewness. The median value might, therefore, be a better parameter of the distribution. If the mean GHQ and GAD score provide a rough guide to the best threshold, then the median of the GHQ and GAD score should give a more reliable guide than the mean. The percentage of completion rates for GHQ-28(M) and GAD-6 components were median (range) 89.7% (82.3-91.2) and 81.5% (77.2-86.3) respectively. From Figures 5 and 6 we concluded that approximately 37% of our student population now faced considerable general health difficulties and only 5% were suffering from serious general anxiety disorder.
Analysis of qualitative data (Thematic analysis): The core categories that emerged during coding using grounded theory [23] are discussed below with supporting statements. The issues surrounding online/remote learning was a dominant theme that emerged and its sub-categories are listed in (Table 3).
Discussion
In our study, there were 64.8% male respondents, their age ranged from 15 to 19. A study conducted by Islam et al. [24] in Bangladesh, showed around 60% (59.5%) of the participants were male, and mean age was 21.4 years (SD=2.0), ranging from 18 to 29 years which support our study findings. In another study done by Begum et al. in Bangladesh found that out of total 1092 participants most of the respondents were male: 732 (67.4 %), and rest were female. This also supported findings of our study [25].
Our study observed that there were various funding sources like family fund, sponsorship from donor agencies, self funded education, student loan from different finance sources, government fund etc (Figure 2). Study conducted by Islam et al. [24]. in Bangladesh, showed students of private Institutions did not need any financial help during this epidemic and spent more time on internet. On the other hand, study pressure was high among the students of public institutions, and they spent less time on internet. They also sought financial help for their study. Besides, most of them did not have any large-screen device like desktop or laptop study done by Begum et al. [25] students of public universities of Bangladesh showed that 550(50.4%) respondents did not bear any portion of their educational or general living expenses. However, 138(12.6%) of respondents replied that their educational or general living expenses were fully borne by themselves and 404(37.0%) of the respondents partially had to bear it.
A bulk of students (51.7%), in our study stated that the quality of education they were receiving during pandemic period were lower compared to the period prior to the pandemic. A majority (59.7%) of students found it difficult to adapt to new teaching methods (zoom classes, online course, online assignment submission and so on) and 37% felt stressed at levels higher than pre pandemic period. Additionally, 42.4% of participants did not have an allocated personal tutor, and of those who did, 7.2% did not get supported by their personal tutor.
In our study, approximately 37% of our student population faced considerable general health difficulties and only 5% are suffering from serious anxiety disorder. These findings were supposed to motivate universities to take immediate proactive measures to identify and mitigate the health issues faced by the students during this pandemic or any future pandemic.
Study done by Son et al. [26] at a public university of USA showed that out of 195 college student participants, 138(71%) indicated that their stress and anxiety had increased due to the COVID-19 pandemic, whereas 39(20%) indicated it remained the same and 18(9%) mentioned that the stress and anxiety had actually decreased. Among those who perceived increased stress and anxiety, only 10(5%) used mental health counseling services. A vast majority of the participants (n=189,97%) presumed that other students were experiencing similar stress and anxiety because of COVID-19. Findings from the international study in which our (Bangladesh) study [20] was a part, observed that 51.4% of university student respondents were suffering from general health challenges according to the GHQ-28 (M), and nearly one third of students (30.9%) were suffering from moderate to severe GAD. These findings were much higher than our (Bangladesh part) study findings.
According to literature search, stress levels reported by Chinese students were much lower early in the pandemic [27]. A cross sectional survey at the University of Texas, USA reported values similar to our parent study [28]. In France the percentage of students suffering from anxiety and depression were 39.19% and 43% respectively [29]. Another study from the UAE on medical and non-medical students also reported levels of anxiety comparable to our parent study [30].
Important features noted from participants’ opinion from thematic analysis were a) Increased quality of learning due to internet access and scope with the new modules b) Digital unavailability due to low middle income of the society as a whole c) Poor interaction with lecturers and peers. d) Inconvenient and insufficient lectures and materials provided through online e) Disparity between teaching and assessment. f) Financial challenges confronting students and their families.
Through thematic analysis majority participants also suggested the following important needed steps a) Ensure library resources to be more easily accessible b) Accessibility of user friendly software. c) Continuing online examinations and assessment d) Induction sessions for students to access digital resources. Outcome of thematic analysis in our study were fairly similar to that in the parent study [20] .
Limitations
Due to the anonymity of the study participants, it was not possible to verify that all participants were students. The questionnaire relied upon trust and honesty. Modification of standard GHQ-28 and GAD-7 instruments might have affected valid
Conclusion
Globally, like in Bangladesh, the general population was affected by COVID -19 pandemic from a socio-economic perspective and students faced further uncertainty with the virtual education reform [31]. When considering the epidemiology of mental health problems among worldwide students pursuing higher education particularly in Bangladesh it was important to pay attention both to assessment of subclinical distress and to diagnoses of major mental illness. Socio demographic factors associated with symptoms including gender, social class must be kept under consideration. Many students were suffering from general health difficulties and general anxiety disorders during COVID-19 pandemic and only a few were accessing appropriate support services.
This study could be an eye opener for planners of nationwide university education at highest Govt. level of Bangladesh during a pandemic like that of COVID -19. Universities and other educational institutions must take proper measures to meet the health needs of their students and mitigate predisposing issues related to virtual education, staff integration and plausible examination formats for future pandemics to come.
Competing interests: There is no conflict of interest. No part of the study has been ever presented or published anywhere.
References
- World Health Organization. Coronavirus disease (COVID-19) pandemic. 2020. https://www.who.int/emergencies/diseases/novelcoronavirus-2019.
- Time. World Health Organization Declares COVID-19 a “Pandemic.” Here’s What That Means. 2020. https://time.com/5791661/who-coronavirus-pandemic-declaration.
- Ferdous MZ, Islam MS, Sikder MT, Mosaddek ASM, ZegarraValdivia JA, Gozal D. Knowledge, attitude, and practice regarding COVID-19 outbreak in Bangladesh: an online-based cross-sectional study. PLoS One. 2020; 15: 0239254. doi: 10.1371/journal.pone.0239254.
- Dutta S, Smita MK. The Impact of COVID-19 Pandemic on Tertiary Education in Bangladesh: Students’ Perspectives. Open Journal of Social Sciences > Vol.8 No.9. 2020.
- Rubin GJ, Wessely S. The psychological effects of quarantining a city. BMJ. 2020; 368: 313. doi:10.1136/bmj.m313.
- Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet. 2020;395 : 912–920. doi :10.1016/S0140-6736(20)30460-8
- Boyraz G, Legros DN. Coronavirus disease (COVID-19) and traumatic stress: probable risk factors and correlates of posttraumatic stress disorder. J Loss Trauma. 2020; 1-20. doi:10.1080/15325024.2020.1763556.
- Islam MS, Akter R, Sikder T, Griffiths MD. Prevalence and factors associated with depression and anxiety among first-year university students in Bangladesh: a cross-sectional study. Int J Ment Health Addict. 2020. doi:10.1007/s11469-020-00242-y.
- Centers for Disease Control and Prevention. Outbreaks can be stressful. 2020. https://www.cdc.gov/coronavirus/2019-ncov/daily-life-coping/managing-stress-anxiety.html.
- World Health Organization. Mental health and psychosocial considerations during the COVID-19 outbreak. 2020. https://www.verywellmind.com/protect-your-mental-health-during-quarantine-4799766.
- Mamun MA, Hossain MS, Griffiths MD. Mental Health Problems and Associated Predictors Among Bangladeshi Students. Int J Ment Health Addict. 2019. doi:10.1007/s11469-019-00144-8.
- Islam MS, Akter R, Sikder T, Griffiths MD. Prevalence and factors associated with depression and anxiety among first-year university students in Bangladesh: a cross-sectional study. Int J Ment Health Addict. 2020. doi:10.1007/s11469-020-00242-y.
- Abdel Wahed WY, Hassan SK. Prevalence and associated factors of stress, anxiety and depression among medical Fayoum University students. Alexandria J Med. 2017; 53: 77-84. doi: 10.1016/j.ajme.2016.01.005.
- Brenneisen Mayer F, Souza Santos I, Silveira PSP, Itaqui Lopes MH, de Souza ARND, Campos EP, et al. Factors associated to depression and anxiety in medical students: a multicenter study. BMC Med Educ. 2016; 16: 282. doi:10.1186/s12909-016-0791-1.
- Saeed H, Saleem Z, Ashraf M, Razzaq N, Akhtar K, Maryam A, et al. Determinants of anxiety and depression among university students of Lahore. Int J Ment Health Addict. 2018; 16: 1283-1298. doi:10.1007/s11469-017-9859-3.
- 16 ul Haq MA, Dar IS, Aslam M, Mahmood QK. Psychometric study of depression, anxiety and stress among university students. J Public Health (Bangkok). 2018; 26: 211-217. doi:10.1007/s10389-017-0856-6.
- UN News. Startling disparities in digital learning emerge as COVID-19 spreads: UN education agency. 2020. [Online]. Available: https://news.un.org/en/story/202 0/04/1062232 Accessed: 2020.
- Devkota P, Rejve K, Janoch E. Bangladesh’s COVID-19 multi-sector impact report: Some insights;2020. :https://usaidlearninglab.org/labnotes/bangladesh%E2%80%99s-covid-19-multisector-impactreport-some-insights Accessed: 1 August 2020
- Uddin M. Effects of the pandemic on the education sector in Bangladesh; 2020. [Online]. https://thefinancialexpress.com.bd/views/effects-of-the-pandemic-on-theeducation-sector-in-bangladesh-1592061447 Accessed: 1 August 2020.
- Gareeb A, Gavazzi I, Woodman N, Goonasekera C, Lombard, Faruq MO et al. A students perspective on University education and wellbeing: one year into the COVID -19 pandemic. Int J Med Stud. 2022; 10: S-219.
- Goldberg DP, Hillier VF . A scaled version of the General Health Questionnaire. Psychological Medicine. 1979; 9: 134-45.
- Spitzer RL, Kroewnke K, Williams JBW, Lowe B. A brief measure for assessing generalized anxiety disorder. The GAD-7. Arch Intern Med. 2006; 1092-1097.23.
- Strauss AL, Corbin JM. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theaory, Sage Publications, Inc. 1998.
- Islam MS, Sujan MSH, Tasnim R, Sikder MT, Potenza MN, vanOs J. Psychological responses during the COVID-19 outbreak among university students in Bangladesh. PLoS One. 2020; 15(12): e0245083. Published 2020 Dec 31. doi: 10.1371/journal.pone.0245083.
- Begum F, Hossain SZ, Alam MS, Islam UN, Lemon HA, Omar NB. Combating the impact of COVID- 19 on Public University Students through Subsidized Online Class: Evidence from Bangladesh. Journal of Education and Practice. 2020; 11(27): 141-50.
- Son C;Hegde S; Smith A; Wang X; Sasangohar F. Effects of COVID-19 on College Students’ Mental Health in the United States: Interview Survey Study. J Med Internet Res 2020; 22(9): e21279. doi: 10.2196/21279.
- CaoW., Fang Z., Hou G., Han M., Xu X., Dong J. & Zheng J. The psychological impact of the COVID-19 epidemic on college students. China.Psychiatry research, 112934. 2020.
- Wang X., Hegde S., Son C., Keller B., Smith A. & Sasangohar F. b. Investigating mental health of US college students during the COVID-19 pandemic: Cross-sectional survey study. Journal of medical Internet research. 2020; 22: e22817.
- Essadek A. & Rabeyron T. Mental health of French students during the Covid-19 pandemic. Journal of affective disorders. 2020; 277: 392-393.
- Saddik B., Hussain A., Sharif-Askari FS., Kheder W., Temsah MH., Koutaich RA, Haddad ES., Al-Roub N M., Marhoon FA. & HAMID, Q. Increased levels of anxiety among. Medical and non-medical university students during the COVID-19 pandemic in the United Arab Emirates. medRxiv. 2020.
- Serafini G., Parmigiafini B., Amerio A., Aguglia A., Sher L. & Amore M. The Psychological impact of COVID-19 on the mental health in the general population. QJM: An International Journal of Medicine. 2020; 113: 531-537.