SciBase Journals
SciBase Epidemiology and Public Health
ISSN 2996-4555
- Article Type: Research Article
- Volume 2, Issue 1
- Received: Oct 23, 2023
- Accepted: Feb 09, 2024
- Published Online: Feb 16, 2024
Satisfaction Level of Multi-Drug Resistant Tuberculosis Patient: A Hospital Based Study in Bangladesh
Md. Abu Sayem1; Md. Khalilur Rahman Khan2; Md. Ashaque Husain3; SM. Abu Zahid4; Md. Mojibur Rahman5; Md. Golam Hossain6*
1University Research Co. (URC), Dhaka, Bangladesh.
2Ministry of Liberation War Affairs, Dhaka, Bangladesh.
3Ministry of Health and Family Welfare, Dhaka, Bangladesh.
4Management Sciences for Health, Dhaka, Bangladesh.
5Bangladesh University of Health Sciences, Dhaka, Bangladesh.
6Department of Statistics, Health Research Group, University of Rajshahi, Rajshahi-6205, Bangladesh.
*Corresponding Author: Md. Golam Hossain
Department of Statistics, Health Research Group, University of Rajshahi, Rajshahi-6205, Bangladesh.
Email: hossain95@yahoo.com
Abstract
Background: Realizing the patients’ need and improving the quality of services, a satisfaction survey can effectively help management and the patient. The aim of this study was to investigate satisfaction level of multi-drug resistant tuberculosis (MDRTB) patients at tertiary level hospital in Bangladesh.
Methods: A cross-sectional study conducted at Chest Disease Hospital (CDH), Rajshahi among 199 MDR-TB patients using random sampling technique. A semi-structured questionnaire was used to collect basic, socio-demographic, behavioral and satisfaction specific data with ensuring no any risk for providing right information. Five point “Likert Scale” was used to measure patients’ satisfaction level. The relevant data were carefully coded and recoded for statistical analysis, and independent samples t-test and multinomial logistic regression analysis were used to see the difference and association of influencing factors on satisfaction.
Results: In this study, we observed that the mean age of MDR-TB patient admitted at CDH was 39.8 years with range from 16 to 62 years. About 90% patients were satisfied with behavior of care providers, and 50% and 29% patients were satisfied in hospital environment and supplied food respectively. We also found that old age group, male, less educated, smoker, diabetic, married, high income and less expenditure group, business or service holder and Muslim were more satisfied than their counterparts. The multinomial logistic regression analysis showed that young age group (≤40 years) was five times more dissatisfied than old age group (≥40 years) (OR=5.345; 95% CI: 1.123-25.448; p<0.05). Receiving monthly money from the program positively impacted on satisfaction. Similarly, drug toxicity, length of stay and loneliness was negatively impacted on satisfaction.
Conclusion: Considering the mentioned influencing factors can strengthen the national control program effort at CDH in Rajshahi division, Bangladesh. Similar study in other chest disease hospitals located mostly in different divisions in the country can also help comparing the factors for nationwide improvement.
Keywords: Satisfaction level; MDR-TB patients; Chest disease hospital; Likert scale; Bangladesh.
Citation: Sayem A, Khan KR, Husain A, Zahid A, Hossain G, et al. Satisfaction Level of Multi-Drug Resistant Tuberculosis Patient: A Hospital Based Study in Bangladesh. SciBase Epidemiol Public Health. 2024; 2(1): 1017.
Introduction
Patients’ satisfaction at hospital level can assume the quality and brand image of the institute [1,2]. Measuring satisfaction can also help reviewing the system, assessing the needs for distribution of resources, reform or modify the process for improvement [3-5]. Along with quality of services covering treatment with cooperation, counseling, time and cleanness, a variety of factors are linked to patients’ satisfaction including socio-demographic and socio-economic condition [6]. However, studies summarized the factors into two broad categories which are mostly influencing the patient’s satisfaction such as providers related and patient related factors [7-9]. In Bangladesh, the provider’s behavior significantly influence patient’s satisfaction [10]. Similarly, presence or visiting of family members, friends or relatives improve patient’s psychological stability and satisfaction level through covering basic needs [11]. Alternatively, many of the factors can augment the patient’s dissatisfaction. Along with effect of present disease, some drugs, some associated diseases and some personal or behavioral factors thus causing depression may instigate or contribute to patient’s dissatisfaction such as anti-TB drugs, diabetes and smoking behavior [12-15]. Furthermore, culture, education, economic condition and country health system can influence satisfaction with realization of the context and resources available [8,16]. Subsequently, due to variation of needs and expectation, the influencing factors of satisfaction may be different in developed and developing countries. On the other hand, patient’s satisfaction is an important index of quality of care in developed countries whereas satisfaction issues and patient’s feedback is often overlooked by the management in developing countries [17-20]. The satisfaction is also depend on different age group and gender [17]. In developing countries like Bangladesh, patients are more satisfied in private hospitals than government or public hospitals while ignoring the cost [21,22]. Some of NGOs are also ensuring quality of services with low cost targeting low and middle income group patient [23]. They are mostly working in rural area of Bangladesh. However, some NGOs are also working in urban city corporation areas under the project “urban primary health care service delivery project (UPHCSDP)” targeting poor urban people [24]. In addition, along with medical university hospital, medical college hospitals, district and sub-district level hospitals, Bangladesh has some government specialized hospitals particularly for cancer, cardiovascular disease, eye, ENT, mental hospitals and others including infectious disease hospitals. The infectious disease hospitals are mostly run in collaboration with NGOs. In Bangladesh, there are 44 chest disease clinics, 6 chest disease hospitals and 7 infectious disease hospitals from where people are receiving both indoor and outdoor services except chest disease clinics where only outdoor services are available [25,26]. These facilities are ensuring respiratory disease screening, detection, treatment and management services with particular emphasis on tuberculosis. The chest disease hospitals are the reference hospitals at regional level where both drug susceptible and drug resistant tuberculosis patients are receiving inpatient and outpatient services. However, under the programmatic management of drug resistant tuberculosis (PMDT), the multi-drug resistant tuberculosis (MDR-TB) patients are mandatory staying in chest disease hospitals for at least four months’ time to accomplish intensive phase of treatment [27]. Perhaps, without surgical or chemotherapy intervention, this is the longest time to stay at hospital for treatment. The length of stay in a hospital is another crucial factor that negatively impact on patient’s satisfaction [28]. We conducted the study at CDH, Rajshahi covering more than sixteen districts of north-west part of Bangladesh from where MDR-TB patients are getting treatment irrespective of economic status, age, gender, ethnicity, occupation or social status. In Bangladesh, several studies on patient satisfaction was conducted at exit level, outpatient level, inpatient with short term stay, compared between public and private hospitals. To the best of our knowledge, there are no any studies on satisfaction level among MDR-TB patients with Bangladeshi population. Hence, the aim of this study was to investigate influencing factors of satisfaction of MDR-TB patients at CDH in Rajshahi division, Bangladesh.
Methods
Study design and study population: A cross sectional study was conducted among 199 multi-drug resistant tuberculosis patients while on treatment at chest disease hospital (CDH), Rajshahi, Bangladesh. As each patient was stayed at CDH for at least four months’ time period to cover intensive phase of treatment, data were collected regularly at four months’ interval from April 2014 to September 2017. The average about 15-35 MDR-TB patients were available in each data collection visit schedule. The face to face interview was conducted by first author to avoid the chance of bias by data collector, patient or by hospital administrator. It is noted that patients were primarily detected or presumed MDR-TB in different facilities of sixteen districts of Rajshahi and Rangpur divisions who were referred to CDH, Rajshahi for confirmation and initiation of treatment through admission at the hospital. There is no authorized alternative private or NGO hospitals for management of MDR-TB in this region.
Study settings and context: CDH is a 150 bedded regional level hospital where TB screening, detection, drug susceptibility testing, testing of non-tubercular mycobacteria (NTM) and other tests opportunity is available in diagnostic unit called “regional TB reference laboratory (RTRL)”. It has both outdoor and indoor services. For indoor services, 50 beds are allotted for MDR-TB patients and remaining 100 beds are for drug susceptible TB patients. Along with government doctors, nurses, laboratory attendant, medical technologist – laboratory (MT Lab.) and other support staffs, the Damien Foundation staffs are actively supporting in diagnostic, follow-up, record keeping and reporting arears. The Damien Foundation is an international non-government organization (NGO) has been working at CDH since long. They are supporting to CDH administration in various areas such as reporting, informing follow-up tests results and so on. However, along with free drugs, diagnosis, treatment and follow-up care, CDH provided food to MDR-TB patients for three times daily which containing roti/bread, rice, meat/fish, vegetables, lentil soup, egg, sugar, milk or banana. In addition, under the programmatic management of drug resistant TB (PMDT), Bangladeshi taka 1000 (equivalent to USD. 12) was given to patients per month to purchase food as diet choice. Some reading books (i.e. novel, life history of famous persons), playing elements (i.e. ludu, carom) and TV was available as recreation materials. Doctors, nurses and support staffs were regularly performed roster duty to regularly monitor treatment progress including drug adverse effect. As infectious disease hospital, it is somewhat isolated from urban gathering and located at the end area of urban premises.
Inclusion/exclusion criteria: Almost all MDR-TB patients were selected except children MDR-TB who were below 15 years of age; and drug susceptible TB patients stayed in separate words. No cases were ignored.
Data collection procedure: Before collection of data, to get right information, patients were properly motivated with assurance that they will not face any situation or difficulties, if they provide right information. Subsequently, first author was also careful to get sensitive information. However, along with basic information, socio-demographic and socio-economic data, personal and behavior related data, disease related expenses, family cooperation, food, provider’s attitude and service related data were collected using pre-tested semi-structured questionnaire. Some open ended questions were included to get comments or opinion or recommendations for the benefits of future patient. Then data were compiled, collated, sorted, coded, recoded and analyzed. Due to scarcity of patients with critical form of disease, 199 patient’s data were randomly collected in four years’ time period. In this study, each respondent had the freedom to share their root causes of satisfaction and dissatisfaction while on taking data in an isolated space, a few meter distances from words or cabins. The purpose was to assure about no harm or risk from hospital administration and to ensure environment for sharing write information spontaneously without fear and hesitation.
Sampling technique: Two-stage stratified random sampling technique was done for selecting male and female patient. First, we selected words and cabin for male and female respectively. Then we selected 131 male and 68 female patients randomly from different words and cabins.
Study variable: Patient’s satisfaction was the major outcome variable for this study. The five-point “Likert Scale” was used to measure satisfaction level which was categorized as 1=highly dissatisfied, 2=satisfied, 3=neutral, 4=satisfied and 5=highly satisfied. The three broad areas were considered for measuring outcome namely (i) provider’s behavior, (ii) hospital environment and (iii) supplied food. In addition, other patient related causal and confounding factors of satisfaction such as smoking, diabetes, expense, family support was also measured.
Statistical analysis: Statistical Package for Social Sciences (SPSS), IBM version 23.00 was used for data analysis. In this study, independent sample t-test and regression analysis was used to see the association and effect of socio-demographic, behavioral and other factors on satisfaction. The value p<0.05 was considered as statistically significant.
Results
Out of 199 respondents, 65.8%, 80.4% and 85.4% was male, married and Muslim respectively. The mean age of patient was 39.8 years with age range from 17 years to 62 years. Independent samples t-test was done to see the difference of satisfaction level by patients’ different socio-demographic factors. We found that, the patients aged >40 years were more satisfied than young patients (≤40 years). Subsequently, male, business or service holder and smoker were significantly (p<0.05) satisfied than their counterparts. The higher income and less expenditure group, less educated (<secondary) patients, married, diabetic and Muslim was more satisfied than their counterparts (p>0.05). Surprisingly, according to behavioral factors, smokers were significantly satisfied than non-smoker (Table 1).
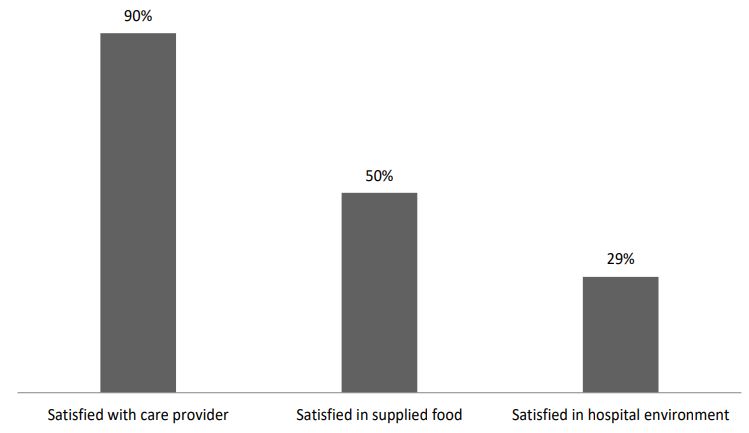
In this study, we measured various factors of satisfaction. Of them, three broad areas and overall satisfaction was analyzed following five point “Likert scale”. We found that, 90% patients were satisfied with provider’s behavior (4.28±0.969). Subsequently, 50% and 29% patients were satisfied in hospital environment and supplied food (main meal) respectively (Figure 1).
Table 1: Difference in satisfaction level of patients by patient’s socio-demographic characteristics (n=199).
| Variable | Mean±SD | p-value | 95% CI of the difference | |
|---|---|---|---|---|
| Age in years | Lower value | Upper value | ||
| ≤40 | 3.46±.848 | 0.006 | -0.563 | -0.095 |
| ≥41 | 3.79±.809 | -0.562 | -0.096 | |
| Gender | ||||
| Male | 3.73±.878 | 0.006 | 0.098 | 0.588 |
| Female | 3.38±.734 | 0.111 | 0.575 | |
| Education | ||||
| <Secondary | 3.63±.831 | 0.603 | -0.176 | 0.303 |
| ≥Secondary | 3.57±.868 | -0.178 | 0.305 | |
| Marital status | ||||
| Married | 3.66±.817 | 0.103 | -0.050 | 0.542 |
| Unmarried | 3.41±.938 | -0.082 | 0.574 | |
| Occupation | ||||
| Hard labor | 3.52±.776 | 0.029 | -0.524 | -0.028 |
| Service or business | 3.79±.946 | -0.541 | -0.011 | |
| Monthly income | ||||
| ≤10000 tk. | 3.56±.834 | 0.335 | -0.355 | 0.122 |
| >10000 tk. | 3.67±.860 | -0.357 | 0.123 | |
| Smoking status | ||||
| Yes | 3.78±.836 | 0.005 | 0.102 | 0.567 |
| No | 3.45±.825 | 0.102 | 0.567 | |
| Diabetes status | ||||
| Yes | 3.73±.654 | 0.259 | -0.120 | 0.444 |
| No | 3.57±.892 | -0.078 | 0.402 | |
| Religion | ||||
| Muslim | 3.61±.858 | 0.881 | -0.310 | 0.361 |
| Non-Muslim | 3.59±.780 | -0.296 | 0.347 | |
| Expenditure | ||||
| 1000-4000 tk. | 3.74±0.853 | 0.114 | 3.53 | 3.95 |
| 5000-7000 tk. | 3.49±0.770 | 3.33 | 3.64 | |
| >7000 tk. | 3.73±1.008 | 3.37 | 4.08 | |
More than 22% and 9% patients were neutral on mentioned areas. However, more than 58% patients were overall satisfied (3.61±0.845). A considerable portion of patients (>31%) were neutral on overall satisfaction (Table 2).
Table 2: Satisfaction score following five-point “Likert Scale” on three broad areas and overall score.
| Satisfaction area | No. of respondent (%) | Mean±SD | |
|---|---|---|---|
|
Satisfied with provider’s behavior |
Highly dissatisfied | 5 (2.5) | 4.28±0.969 |
| Dissatisfied | 14 (7.0) | ||
| Neutral | 1 (0.5) | ||
| Satisfied | 80 (40.2) | ||
| Highly satisfied | 99 (49.8) | ||
|
Satisfied with hospital environment |
Highly dissatisfied | 7 (3.5) | 3.19±1.017 |
| Dissatisfied | 54 (27.1) | ||
| Neutral | 44 (22.1) | ||
| Satisfied | 82 (44.2) | ||
| Highly satisfied | 12 (6.0) | ||
|
Satisfied with supplied food |
Highly dissatisfied | 13 (6.5) | 2.55±1.013 |
| Dissatisfied | 120 (60.3) | ||
| Neutral | 18 (9.0) | ||
| Satisfied | 40 (20.1) | ||
| Highly satisfied | 8 (4.0) | ||
| Overall satisfied | Highly dissatisfied | 0 (0.0) | 3.61±0.845 |
| Dissatisfied | 21 (10.6) | ||
| Neutral | 62 (31.2) | ||
| Satisfied | 90 (45.2) | ||
| Highly satisfied | 26 (13.1) |
The multinomial logistic regression analysis showed that young age group (≤40 years) was five times higher dissatisfied than adult or old age group (≥40 years) (OR=5.345, 95% C.I: 1.123-25.448; p<0.05). It means that the younger patients had higher probability to get bad experience in the hospital. Consequently, the analysis depicted the summery of satisfaction on different co-variates where the highly satisfied was the reference value. In this study, both lower and middle expenditure groups were around five times higher satisfied than higher expenditure group (OR=4.805, 95% C.I: 1.258-18.349; p<0.05 and OR=5.214, 95% C.I: 1.390-19.559, p<0.05) (Table 3).
Table 3: Multinomial logistic regression factors influencing of satisfaction level (N=199).
| Variables | Satisfaction Level | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Dissatisfied | Neutral | Satisfied | |||||||
| p-value | OR | 95% CI for OR | p-value | OR | 95% CI for OR | p-value | OR | 95% CI for OR | |
| Gender | |||||||||
| Male | 0.388 | 0.402 | 0.051-3.190 | 0.086 | 0.193 | 0.030-1.262 | 0.131 | 0.246 | 0.040-1.518 |
| Female | - | - | - | - | - | - | - | - | - |
| Age in years | |||||||||
| ≤40 | 0.035* | 5.345 | 1.123-25.448 | 0.074 | 3.056 | 0.898-10.402 | 0.105 | 2.600 | 0.820-8.245 |
| ≥41 | - | - | - | - | - | - | - | - | - |
| Religion | |||||||||
| Muslim | 0.405 | 0.418 | 0.054-3.256 | 0.498 | 0.543 | 0.093-3.175 | 0.334 | 0.444 | 0.086-2.302 |
| Non-Muslim | - | - | - | - | - | - | - | - | - |
| Marital status | |||||||||
| Married | 0.423 | 0.506 | 0.096-2.670 | 0.781 | 1.241 | 0.270-5.712 | 0.824 | 1.177 | 0.279-4.972 |
| Non-Married | - | - | - | - | - | - | - | - | - |
| Smoking status | |||||||||
| Yes | 0.352 | 0.471 | 0.097-2.299 | 0.898 | 1.090 | 0.289-4.105 | 0.856 | 1.119 | 0.333-3.761 |
| No | - | - | - | - | - | - | - | - | - |
| Education | |||||||||
| <Secondary | 0.198 | 0.377 | 0.085-1.667 | 0.315 | 0.534 | 0.157-1.815 | 0.179 | 0.456 | 0.145-1.433 |
| ≥Secondary | - | - | - | - | - | - | - | - | - |
| Occupation | |||||||||
| Hard Labor | 0.132 | 3.493 | 0.686-17.796 | 0.013* | 5.297 | 1.416-19.816 | 0.043* | 3.458 | 1.041-11.487 |
| Service & Business | - | - | - | - | - | - | - | - | - |
| Income in BDT. | |||||||||
| ≤10,000 | 0.301 | 2.245 | 0.484-10.409 | 0.753 | 1.221 | 0.352-4.240 | 0.729 | 1.233 | 0.378-4.022 |
| >10,000 | - | - | - | - | - | - | - | - | - |
| Expenditure in BDT. | |||||||||
| 1000-4000 | 0.193 | 3.166 | 0.558-17.979 | 0.663 | 1.392 | 0.315-6.150 | 0.022* | 4.805 | 1.258-18.349 |
| 5000-7000 | 0.256 | 2.674 | 0.489-14.612 | 0.012* | 5.713 | 1.458-22.385 | 0.014* | 5.214 | 1.390-19.559 |
| ≥8000 | - | - | - | - | - | - | - | - | - |
a. The reference category: Highly satisfied, Note: * p<0.05, OR: Odds ratio.
In this study, more than 26% patients were happy to get money from hospital instead of paying hospital charge. A portion of patients (22%) were satisfied with hospital management (i.e. gossiping, reading, TV watching opportunity with good living arrangement). The remaining percentage of patients were satisfied with provider’s behavior (>9%), counseling system (7%), nutritious food and fruits (8%), improving health condition (13%), high cooperation with no cost (7%) and others (Table 4). Alternatively, more than 22% patients showed dissatisfaction that arises mainly due to depart from family. They expressed as feeling alone, confined in a hospital room without family, missing their children. Around 27% patients showed their bad feelings or dissatisfaction on drug toxicity which was expressed as after taking drugs, they felt very uneasy. More than 20% patient was concentrated on their weakness as root cause of their dissatisfaction. Among the respondents, 5% voluntarily reacted on supplied food and more than 10% on hospital environment. Around 13% reacted that they perceived non-cooperation of nurses and support staffs that made them dissatisfied (Table 4). A significant portion of respondent shared their family member’s visits with showing positive and negative emotional expression. This study revealed that more than 80% patients received family support and cooperation. The family members were visiting them with frequency from 1 time to more than 20 times per month. Even around 16% family members were living with them for ensuring daily care and mental support. On the other hand, 19% patients expressed that their family members did not come to see them in last month (Table 4). Subsequently, 16% patients emotionally expressed that they were willing to return back to home before completion of full course of treatment (Table 4).
Table 4: Expression of satisfaction, dissatisfaction and emotion by hospital admitted patients. n=199.
| Causes of satisfaction | Number | % |
|---|---|---|
| 1. Good living arrangement compared to other government hospitals | 20 | 10.0 |
| 2. Doctors and other staffs are cooperative and supportive | 19 | 9.5 |
| 3. Sometimes administrator and higher level health authorities are coming to meet us and showing empathy with counseling | 4 | 2.0 |
| 4. A variety of counseling system giving me hope of survival | 10 | 5.0 |
| 5. Here, there is playing, gossiping, reading books and TV enjoying opportunity which is exceptional at government hospital level | 24 | 12.1 |
| 6. Enjoying fruits like banana, milk, sugar, egg, bread daily beyond cocking meal | 16 | 8.0 |
| 7. Getting free treatment, no service charge, no support staff’s charge or hospital charge, even getting tk. 1000 per month | 40 | 20.1 |
| 8. Interesting that, I am getting money from hospital instead of paying hospital charge | 12 | 6.0 |
| 9. Getting good quality services with very minimum cost, only travel cost | 14 | 7.0 |
| 10. Gradually improving health condition | 26 | 13.1 |
| 11. Here, I have got friends with same health condition | 9 | 4.5 |
| 12. My family is making me happy and caring me more | 5 | 2.5 |
| Causes of dissatisfaction | ||
| 1. Feeling alone in the hospital | 3 | 1.5 |
| 2. Confined in a room, living here without family | 22 | 11.1 |
| 3. Feeling alone, missing children, neighbors, friends and relatives | 20 | 10.1 |
| 4. After taking medicine, feeling very uneasy | 53 | 26.6 |
| 5. Often feel weak | 40 | 20.1 |
| 6. Unhygienic toilet, words are not properly clean, no regular changing of bedsheets | 10 | 5.0 |
| 7. Everyday same food, hybrid food, bad taste, lack of toilet hygiene, no regular cleaning of words, changing of bedsheets | 11 | 5.5 |
| 8. Nurses and support staffs sometimes shows non-cooperation | 26 | 13.1 |
| 9. Very long treatment time at hospital level | 5 | 2.5 |
| 10. Inadequate freedom of outside movement even at hospital premises, restricted smoking | 9 | 4.5 |
| Family member’s visit frequency per month | ||
| 1-5 times | 10 | 5.0 |
| 6-10 times | 57 | 28.6 |
| 11-20 times | 22 | 11.1 |
| 20+ times | 41 | 20.6 |
| Living with me | 31 | 15.6 |
| Not coming | 38 | 19.1 |
| Willing to return home before completion of medication | ||
| Yes | 32 | 16.1 |
| No | 167 | 83.9 |
Discussion
The chest disease hospital (CDH), Rajshahi was following 9th months treatment regimen whereas some national govt. hospitals were following 22-24 months’ regimen for MDR-TB. Both regimens were approved by national tuberculosis control program (NTP) [29]. However, the treatment regimen has two phases called intensive and continuous phase (CP). According to national guidelines of NTP, patients must stay at hospital to complete intensive phase (IP) of treatment. For 9th months regimen, MDR-TB patients were stayed at CDH, Rajshahi for four months’ time to complete IP. The remaining five months were treated at community level. In this study, we found higher prevalence of male and young aged MDR-TB patients which is consistent with other studies in Bangladesh [30-32]. However, our findings demonstrated that young aged were more dissatisfied than middle or old aged people. A various factor such as ability to adoption, realization of context is usually higher among aged people than young people. In addition, aged people might be more experienced in different health facilities to compare the system, process, cost, cooperation, environment and other areas. Different studies also found similar results on association between age and satisfaction [17]. It is noted that there were no alternative options for MDR-TB patients at govt. general or medical college hospitals, private or NGO hospitals to get services in Rajshahi and Rangpur divisions. In CDH, male and female words are separated and majority of patients were living in words. This study showed higher satisfaction among male which may indicate individual word management including cleanness and toilet hygiene. In Bangladesh, males are usually raise voice to get services and support compared to females. Based on realization and review of information, it is assumed that gender difference of satisfaction usually influenced by local management. Hence, the different countries showed different results. A study in Nepal showed females were more satisfied than male [17]. Alternatively, Malaysia and Nigeria showed higher satisfaction among male than female [34,35]. In our study, businessman and service holders were significantly satisfied than hard labor which may indicates inequality or deprivation to get equal services. In CDH, Rajshahi, though the hospital management often counseled on cessation of smoking, a portion of patients were moving to isolated and hidden areas for smoking. We observed an interesting finding that smokers were more satisfied than non-smokers (p<0.05). Our finding is also consistent with other study [36]. We also found higher satisfaction among less educated, married, diabetic, more income and less expenditure group (p>0.05). In spite of drugs adverse effect, lengthy treatment time and other limitations, 58% patients were overall satisfied with >31% neutral. It indicates a good quality of services at CDH, Rajshahi. We followed five-point “Likert Scale” in measuring satisfaction of MDR-TB patients, a group of special type patients. In our study, 90% of the respondents were satisfied with provider’s behavior that indicates an important marker of service quality, cooperation, time spent with patients, sincerity, regularity and performance. In contrast, a study showed 63.2% to 52% satisfaction rate at government level facilities in Bangladesh with recommendation on improvement of interpersonal skills of care providers [8]. The satisfaction level was declined in other two major areas. Among the respondents, 50% patients were satisfied in hospital environment thus indicates the area of improvement. The respondents perceived the necessity of improvement particularly on toilet hygiene, regular cleaning of words and changing of bedsheets. Subsequently, only 29% patients were satisfied in hospital supplied food (two times main meal). It is noted that the patients were receiving breakfast containing one banana and or milk, egg, sugar and bread; lunch and dinner containing lentil soup, fish or meat and vegetables. In addition, under PMDT, patients were receiving BDT. 1000.00 per month to purchase food or fruits from outside as diet choice. Most of the respondent reacted that due to bad taste and same food item daily made them dissatisfied. In CDH, contractor/vendor was providing food items and govt. cock was processing the items. The cock’s job stability and vendor’s agreement for supplies were a noted barrier with other factors. The multinomial logistic regress analysis also showed young age group was five times dissatisfied than their counterpart. The different occupation was listed as agriculture, business, services, students, housewife, fisheries, poultry and others. Finally, occupation was recoded into hard labor and business and services where we found businessman and service holders were 3.5 times higher satisfied than hard labor. A study in Nepal also found agriculture occupation group was less satisfied than service occupation group which is consistent with our finding [17]. Subsequently, less and middle expenditure groups were around five times higher satisfied than high expenditure group. A study in Bangladesh showed similar finding for public hospitals. They described as negative correlation between satisfaction and expenditure in public hospitals [21]. The CDH, Rajshahi is a special type govt. health facility where donor and NGOs have contribution to patient management thus the patients received comparatively higher support than other public hospitals. In our study, patients were asked the reasons of being satisfied or dissatisfied as open questions. They answered with their experience and emotion. Around 10% patients declared that the living arrangement was comparatively better than other govt. hospitals they experienced or observed. The CDH is a 150 bedded hospital both for MDR-TB and drug susceptible TB where average 50-90 patients were available thus they did not face huge rushing, noise and other hazards. A large portion of patients were happy to get money with free treatment. To ensure nutrition, this amount was provided to each patient under PMDT. A specially designed govt. and donor funding (GFATM) program that attracts the patients to continue treatment. As patient need to stay for a long time, management nicely organized the words with health messages, novels and initiated recreational options such as gossiping with other patients, reading a novel or motivational books, watching TV. A significant percentage of patients (>22%) were satisfied with this arrangement. However, patients were satisfied with management, nutritious food and fruits, gradual improvement of health condition and others areas (Table 4). Alternatively, a large portion of patients expressed their loneliness arises mainly due to depart from family. They were not concentrated on management to be dissatisfied. Another portion expressed their dissatisfaction on drug toxicity and weakness. However, 5% reacted on supplied food such as very bad taste, everyday same food, hybrid food, no evening snacks, no improve diet and 10% on hospital environment like lack of toilet hygiene, no regular cleaning of words, no regular changing bedsheets. A portion also perceived non-cooperation of nurses and support staffs (Table 4). Author observed both positive and negative emotional expression while on answering about family member’s visit. During their vulnerable situation, more than 80% patients received family support and cooperation. The family members visited them from 1 time to more than 20 times per month. Even around 16% family members were living with them for ensuring daily care and mental support. Those who come from nearest distance, they visited frequently mostly with home-made food and clean cloths; and those who come from other districts, often a family member, mostly female member for female patient, wife or male member for male patient spent a full time at hospital. On the other hand, more than 19% patients expressed that their family members did not come in last month. Whatever the causes of absenteeism, patients showed negative expression on family support. In this study, more than 16% patients were willing to move to home earlier ignoring the full regimen of treatment at hospital. The drug toxicity, lengthy treatment period and home sleekness made them emotional.
Strength and limitations: As the first author himself collected data, there was no chance of misinterpretation or manipulation of data or chance of any bias by data collectors, hospital administration or patients. In addition, the study was approved by Line Director of NTP, Ministry of Health and Family Welfare, Bangladesh. However, along with strength, we had some limitations. We did not compare with other chest disease hospitals due to time constraints and distance. We did not compare with nearest public, private or NGO facilities where the patients were stayed for a short duration. We did not take any providers feedback against patient’s behavior which would be the potential clues for researchers for further study.
Conclusion
From patient’s perspective, age, gender, occupation and smoking status was considered as significant influencing factors. In addition, education, marital status, religion, diabetes status, income, expenditure, apart from family, home sickness and family member’s visits were also considered as influencing factors. Similarly, from provider’s perspective, provider’s behavior, hospital environment, supplied food were major influencing areas of satisfaction. In addition, counseling system, money from program, lengthy treatment time and drugs toxicity influences patient’s satisfaction and psychological state. The management can review the patient’s feedback for satisfying the patients and improving the quality.
Declarations
Ethics approval and consent to participate: Before collection of data, the author received study approval as well as data collection approval from the authority of line director, TB/Leprosy, ministry of health and family welfare (memo no. 4-90/tb-lep/others/1465) and hospital superintendent (signed on 23/3/2014). The ethical approval was also taken from Institute of Biological Sciences, University of Rajshahi (No: 49/320/ IAMEBBC/IBSC). However, average 15 to 30 MDR-TB patients were available in each data collection schedule. The survey received informed consent from each individual in the study. All methods of the study were performed in accordance with the relevant guidelines and regulations.
Abbreviations: CDH: Chest disease hospital; CI: Confidence interval; CP: Continuation phase; GFATM: Global fund to fight AIDS; tuberculosis and malaria; ENT: Ears; nose and throat; IBM: International Business Machines Corporation; IP: Intensive phase; MDR-TB: Multi-drug resistant tuberculosis; MT Lab.: Medical technologist– laboratory; NGO: Non-government organization; NTM: Non-tubercular mycobacteria; NTP: National tuberculosis control program; OR: odds ratio; PMDT: Programmatic management of drug resistant tuberculosis; RTRL: Regional TB reference laboratory; TB: Tuberculosis; TV: Television; SPSS: Statistical package for social sciences; UPHCSDP: Urban primary health care services delivery project; USD: United States dollar.
Declarations
Consent for publication: Not applicable for this study.
Availability of data and materials: Patient level data will be available on request to corresponding or first author.
Competing interests: The authors declare that they have no competing interests.
Funding: There was no grant, technical or corporate support for this study.
Authors’ contributions: Conceptualization: MAS; Formal analysis: MAS, MGH; Investigation: MGH, MKRK; Methodology: MAS, MGH; Resources: MGH, MKRK, MAH, SMAZ and MMR; Supervision: MGH; Writing- original draft: MAS; Writing- review & editing: MAS, MGH, MKRK, MAH, SMAZ and MMR.
Acknowledgement: The authors would like to thanks to authority of NTP and Chest Disease Hospital, Rajshahi Bangladesh for giving permission and providing necessary information of patients. The authors would also like to express their sincere gratitude to all study participants and the staff engaged in the study.
References
- L Liu, J Fang. Study on potential factors of patient satisfaction: Based on exploratory factor analysis. Patient Prefer. Adherence. 2019; 13: 1983-1994.
- F Farzianpour, R Byravan, and S Amirian. Evaluation of Patient Satisfaction and Factors Affecting It: A Review of the Literature. Health (Irvine. Calif). 2015; 7(11): 1460-1465.
- S Jiang, W min Wu, and P. Fang. Evaluating the effectiveness of public hospital reform from the perspective of efficiency and quality in Guangxi, China. Springerplus. 2016; 5: 1.
- SS Andaleeb. Service quality perceptions and patient satisfaction: A study of hospitals in a developing country. Soc. Sci. Med. 2001; 52(9): 1359-1370.
- EK Mpinga and P Chastonay. Satisfaction of patients: A right to health indicator?. Health Policy (New. York). 100: 2(3): 144-150.
- G Lewis, H Kirkham, I Duncan, and R Vaithianathan. How health systems could avert ‘Triple Fail’ events that are harmful, are costly, and result in poor patient satisfaction. Health Aff. 2013; 32(4): 669-676.
- A Junewicz and SJ. Youngner. Patient-satisfaction surveys on a scale of 0 to 10: Improving health care, or leading it astray?. Hastings Cent. Rep. 2015; 45(3): 43-51.
- G Adhikary, et al. Factors influencing patients’ satisfaction at different levels of health facilities in Bangladesh : Results from patient exit interviews. PLoS One. 2018; 1-13.
- A Donabedian. The Lichfield Lecture. Quality assurance in health care: consumers’ role. Qual. Health Care. 1992; 1(4): 2470-251.
- JM Aldana, H Piechulek, and A Al-Sabir. Client satisfaction and quality of health care in rural Bangladesh. Bull. World Health Organ. 2001; 79 (6): 512-517.
- P Bellou and KG Georgianni. The contribution of family in the care of patient in the hospital. Heal. Sci. J. 2014; 1(3): 1-6.
- A Pachi, D Bratis, G Moussas, and A. Tselebis. Psychiatric Morbidity and Other Factors Affecting Treatment Adherence in Pulmonary Tuberculosis Patients. Tuberc. Res. Treat. 2013; 1-37.
- S. A. K, K. V. K, S RB, and G A. Depression among people living with type 2 diabetes in an urbanizing community of Nepal. PLoS One. 2019;14(6): 0218119.
- C Garrett and A Doherty. Diabetes and mental health. Clin. Med. J. R. Coll. Physicians London. 2014; 14(6): 669-672.
- M Fluharty, AE Taylor, M Grabski, and MR Munafò. The association of cigarette smoking with depression and anxiety: A systematic review. Nicotine Tob. Res. 2017; 19(1): 3-13.
- S Xesfingi, A Vozikis. Patient satisfaction with the healthcare system: Assessing the impact of socio-economic and healthcare provision factors. BMC Health Serv. Res. 2016; 16: 1.
- M Adhikari, NR. Paudel, SR. Mishra, A Shrestha, DP. Upadhyaya. Patient satisfaction and its socio-demographic correlates in a tertiary public hospital in Nepal: a cross-sectional study. BMC Health Serv. Res. 2021; 21: 1.
- Rashid Al-Abri, Amina Al-Balushi. Patient Satisfaction Survey as a Tool towards Quality Improvement. Oman Med J. 2014; 29(1): 3-7.
- A Coulter and PD Cleary. Patients’ experiences with hospital care in five countries. Health Aff. 2001; 20(3): 244-252.
- Ministry of Health, New ERA, and Nepal Helath Sector Support Program (NHSSP) and ICF. Nepal Health Facility Survey 2015. Nepal Minist. Heal. 2015; 51-52.
- F Begum, J Said, SZ. Hossain, MJ. Hasan, and N Binti. Healthcare Cost and Patient Satisfaction: A Comparative Analysis Between Public and Private Hospitals in Bangladesh. Res. 2019; 1-19.
- SA. Syed, S Nazlee, and K Shahjahan. Patient satisfaction with health services in Bangladesh. Health Policy Plan. 2007; 1-11.
- A Mercer, MH Khan, M Daulatuzzaman, and J Reid. Effectiveness of an NGO primary health care programme in rural Bangladesh: Evidence from the management information system. Health Policy Plan. 2004; 19(4): 187-198.
- Asian Development Bank. Bangladesh: Urban Primary Health Care Services Delivery Project. 2017.
- Health Bulletin, MIS, DGHS Bangladesh. 2019.
- Annual report, National Tuberculosis Control Programme, Bangladesh. 2020.
- Government of the People’s Republic of Bangladesh. National Guidelines and Operational Manual for Programmatic Management of Drug Resistant TB (PMDT) National Guidelines and Operational Manual for Programmatic Management of Drug Resistant TB (PMDT). 2013; 1-146.
- W Diwan, PA. Nakonezny, J Wells. The Effect of Length of Hospital Stay and Patient Factors on Patient Satisfaction in an Academic Hospital. Orthopedics. 2020; 43(6): 373-379.
- Annual report, National Tuberculosis Control Program, DGHS, Bangladesh. 2017.
- S Banu, et al. Multidrug-resistant tuberculosis in admitted patients at a tertiary referral hospital of Bangladesh. PLoS One. 2012; 7(7).
- MA Sayem, MG Hossain, T Ahmed, K Hossain, and ZA. Saud. Effect of Nutritional Support on Treatment of Multi-Drug Resistant Tuberculosis in Rajshahi Division, Bangladesh. J. Tuberc. Res. 2020; 08(04): 223-236.
- N Begum, MH. Ansari, H Jahan, and F Akhter. Profile of MDRTB Patients Admitted in a Tertiary Level Hospital in Bangladesh. 2017; 15-19.
- E Batbaatar, J Dorjdagva, A Luvsannyam, and P Amenta. Conceptualisation of patient satisfaction: A systematic narrative literature review. Perspect. Public Health. vol. 2015; 135(5): 243-250.
- K Ganasegeran, W Perianayagam, R Abdul Manaf, SA Ali Jadoo, and S. A. R. Al-Dubai. Patient satisfaction in Malaysia’s busiest outpatient medical care. Sci. World J. 2015.
- B Bener, S Ghuloum. Gender difference on patients’ satisfaction and expectation towards mental health care. Niger. J. Clin. Pract. 2013; 16(3): 285-291.
- LI Solberg, RG Boyle, G Davidson, S Anne Magnan, CL Carlson. Patient satisfaction and discussion of smoking cessation during clinical visits. Mayo Clin. Proc. 2001; 76(2): 138-143.