
SciBase Journals
SciBase Gastroenterology and Hepatology
ISSN 2691-7785
- Article Type: Case Report
- Volume 1, Issue 1
- Received: Jul 08, 2024
- Accepted: Aug 29, 2024
- Published Online: Sep 05, 2024
Synchronous Widely Cutaneous Metastasis from Primary Gastric Cancer: A Case Report
Mehmet Emin Buyukbayram1; Zekeriya Hannarici1; Ali Yılmaz1; Mehmet Bilici1; Salim Başol Tekin1; Numan Bulut2
1Department of Medical Oncology, Atatürk University Faculty of Medicine, Erzurum, Turkey.
2Department of Pathology, Ataturk University Faculty of Medicine, Erzurum, Turkey.
*Corresponding Author: Mehmet Emin Buyukbayram
Department of Medical Oncology, Atatürk University Faculty of Medicine, Erzurum 25100, Turkey.
Tel: +905392449362;
Email: m.eminbuyukbayram@hotmail.com
Abstract
Background: Metastasis from internal neoplasms to the cutaneous is uncommon. They can be metachronous or synchronous. Widely synchronous metastasis from the gastric to the cutaneous is a rare clinical condition.
Case presentation: We reported a male patient with widely synchronous cutaneous metastasis from the gastric at the age of 59 years. Widely metastatic mass as a patch nodüler lesions before the primary gastric tumor diagnosis. Go on biopsy from the skin and gastric carcinoma undifferentiated cells detecting. Vimentin positive and panCK (pan cytokeratin) positive, desmin, SMA (smooth muscle antibody), S-100, CD (cluster of differentiation) 31, CD34, F13a, MyoD1 (myogenic differentiation), CD68 negative in tumoral areas immunohistochemically verified the cutaneous metastasis of gastric adenocarcinoma.
Conclusion: In light of this information, widely cutaneous lesions should be biopsy and make clear metastasis and originate the primer tumor.
Keywords: Cutaneous metastasis; Gastric cancer; Skin cancer.
Citation:Buyukbayram ME, Hannarici Z, Yılmaz A, Bilici M, Başol Tekin S, Bulut N. Synchronous Widely Cutaneous Metastasis from Primary Gastric Cancer: A Case Report. SciBase Gastroenterol Hepatol. 2024; 1(1): 1002.
Introduction
Metastases to the cutaneous are very rare site [1]. All of skin cancer 2% are metastatic and most commonly breast, lung and gastrointestinal tissue tumors with advanced stage and poor prognosis [2,3]. Gastric cancer most metastatic sites are liver, peritoneum and lymph nodes [3]. Gastric cancer metastasis to cutaneous is uncommon, Additionally, metastasis from gastric to cutaneous widely patchy nodular is much uncommon [2]. We reported gastric cancer with widely cutaneous metastasis.
Case Presentation
A married male patient aged 59 years applied to our hospital with a diagnosis of malign tumor positive widely patchy nodular lesions fine needle biopsy for three months history of headache, extensive skin lesions. İn the general examination of patient there were cutaneous lesions on the neck, chest wall and the back (Figure 1C) and the ECOG performance score of patient was two. The patient was having Carcinoembryonic Antigen (CEA): 319 ng/ml( normal, 0-3 ng/ml), Carbohydrate Antigen (CA) 19-9 : 13.8 U/ml ( normal,0-31.3 U/mL), alkaline phosphatase: 122 U/L ( normal 40-120 U/L) and in his laboratory. The fine needle of biopsy from skin lesions; on the surface, keratinized stratified squamous epithelium, infiltrate consisting of neoplastic cells with large hyperchromatic nuclei in the dermal area and neoplastic cells trying to form atypical pleomorphic gland-like structures infiltrated into the dermal area were seen (Figures 1A, 1B).
The patient was detecting for primary tumor which metastases to skin and were on Positron Emission Tomography + Computer Tomography (PET-CT). In PET-CT, besides gastric diffuse hypermetabolic involvement; there were gastrohepatic, celiac, paracaval, paraaortic, parapancreatic Lymph Node (LN) metastasis, bilateral juguler, infraclaviculer, bilateral axillary, anterior mediasten, paratrakeal, carinal, subcarinal LN metastasis and widespread bone metastasis were find. The patient had an upper endosdocopy and central ulceration with vegetan lesion had seen and get biopsy. Neoplastic cells with panCK (pan cytokeratin) positive, musin positive, sinaptofizin negative, kromograninin negative and CD (cluster of differentiation) 56 negative a signet cell adenocarcinoma diagnosed. Localized mitotic figures were observed in the stroma and a tumoral structure consisting of signet ring cells containing intracytoplasmic mucin was also observed (Figure 2). The skin patchy noduler lesion biopsy was malign tumor positive and Vimentin positive, panCK positive, desmin, SMA (smooth muscle antibody), S-100, CD31, CD34, F13a, MyoD1 (myogenic differentiation) and CD68 negative. While the consultation pathology this statement its thought that signet cell adenocarcinoma of gastric tumor which involve undifferation cells, evaluate as a skin metastasis (Figure 2). The FLOT KT protocol was projected for the patient. Clinical respons is has and going on KT.
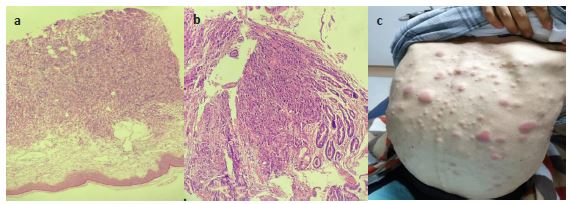
(b) Neoplastic cells attempting to form atypical pleomorphic gland-like structures infiltrating the dermal area (H&E) (x400).
(c) The back of patients and noduler lesions.
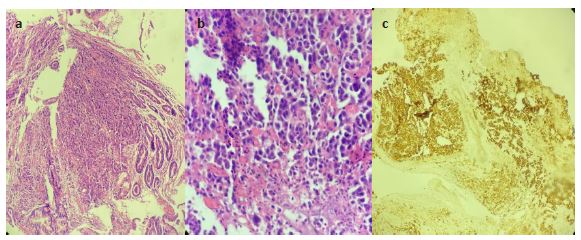
(b) Localized mitotic figures were observed in the stroma and a tumoral structure consisting of signet ring cells containing intracytoplasmic mucin was also observed (H&E) (X400).
(c) Infiltrative glandular structures and single cells (panCK) (X40).
Discussion
Its overall incidence corresponding to 5% of all visceral malignancies, cutaneous metastasis is a rare type of cancer, which commonly originates from breast (the most) as well as lung, colon, oral cavity, kidney, or ovarian malignancies [4-6]. Cutaneous metastasis from gastric cancer is often regarded as incurable in the late stages of advanced cancer [1]. We searched the PubMed database for reports of cases undergoing of cutaneous metastasis from gastric cancer using with the keywords “gastric cancer,” “synchoronus,” and “cutaneous metastasis.” Two cases were found [1,3]. A 89 year old man with only right axillary synchronous metastasis and were on surgery treatment and after late recurrence had. The other review a 60 year old man only above the sternum erythematous lesion synchronously had and were on surgery treatment [1,3]. Gastric metastasis to skin occurs by hematogenous or lymphatic spread, direct invasion of primary cancer, and intraoperative implantation of cancer cells into the skin. In our case, extensive synchronous cutaneous metastasis in the neck, chest wall and back can be explained by hematogenous spread from the primary gastric cancer. Besides extensive skin lesions, there were gastrohepatic, cöliac, paracaval, paraaortic, parapancreatic lymph node metastasis, bilateral juguler, infraclaviculer, bilateral axillary, anterior mediasten, paratrakeal, carinal, subcarinal LN metastasis and widespread bone metastasis.
According to the literature, multiple metastasis to the skin is uncommon [3]. Generally metastases to skin as seen hyperpigmented nodules or erythematous lesion. In our case patchy nodüler lesions and surface on erythema had at the presentation to hospital. The patient were on skin biopsy and malign tumor positive undifferentiation cells detecting. In the immunohistochemical study vimentin positive and panCK positive, desmin, SMA, S-100, CD31, CD34, F13a, MyoD1, CD68 negative. After primer malignancy detecting with PET-CT gastric diffuse hypermetabolic was sign. Endoscopy and gastric biopsy shows adenocarcinoma CerbB2 negative with signet cells. Pathologic consultation make clear that gastric adenocarcinoma tumors undifferentiation cells metastases to skin.
In case of metastasis to the skin, treatment management is not different and multiple metastases and end stage of disease surgery not indicated. According to the recent reports, the management of skin metastases if soliter lesion and local or locally advanced disease can be surgery and rekurrens of metastatic skin disease is high [1]. In our case extensive skin lesions and end stage of the disease we started chemotherapy FLOT and clinically response has.
Conclusion
Gastric cancer and the other internal neoplasms metastasis to skin expected. All of skin metastasis can primate the primer tumor while detecting cancer. Even though gastric cancer has the potential to metastasize to the skin extensive localization, this has rarely been reported in the literature. In patients diagnosed with gastric cancer, the presence of suspicious cutaneous lesions should be verified by biopsy make clear it.
Ethical approval: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Conflict of interest: The authors declare that they have no conflict of interest.
References
- Koyama R, Maeda Y, Minagawa N, Shinohara T, Hamada T. Late Cutaneous Metastasis Originating from Gastric Cancer with Synchronous Metastasis. Case Rep Gastroenterol. 2019; 13(1): 95-101. doi: 10.1159/000497099.
- Gündüz Ö, Emeksiz MC, Atasoy P, Kidir M, Yalçin S, et al. Signet-ring Cells in the Skin: A Case of Late-onset Cutaneous Metastasis of Gastric Carcinoma and a Brief Review of Histological Approach. Dermatol Reports. 2017; 8(1): 6819. doi: 10.4081/dr.2016.6819.
- Cesaretti M, Malerba M, Basso V, Boccardo C, Santoni R, et al. Cutaneous metastasis from primary gastric cancer: a case report and review of the literature. Cutis. 2014; 93(4): E9-E13. PMID: 24818191.
- Krathen RA, Orengo IF, Rosen T. Cutaneous metastasis: A meta-analysis of data. South Med J. 2003; 96(2): 164-7.
- Hu SC, Chen GS, Lu YW, Wu CS, Lan CC. Cutaneous metastases from different internal malignancies: a clinical and prognostic appraisal. J Eur Acad Dermatol Venereol. 2008; 22(6): 735-40.
- Schwartz RA. Cutaneous metastatic disease. J Am Acad Dermatol. 1995; 33(2 Pt 1): 161-82.