
SciBase Journals
SciBase Gastroenterology and Hepatology
- Article Type: Research Article
- Volume 1, Issue 1
- Received: Aug 27, 2024
- Accepted: Oct 02, 2024
- Published Online: Oct 09, 2024
The Bevacizumab Skip in Atezolizumab plus Bevacizumab for Hepatocellular Carcinoma
Kei Amioka1; Kenji Yamaoka1; Hikaru Nakahara1; Shigeki Yano1; Kensuke Naruto1; Yasutoshi Fujii1; Shinsuke Uchikawa1; Hatsue Fujino1; Atsushi Ono1; Takashi Nakahara1; Eisuke Murakami1; Tomokazu Kawaoka1*; Daiki Miki1; C Nelson Hayes1; Masataka Tsuge1,2; Shiro Oka1
1Department of Gastroenterology, Graduate School of Biomedical and Health Sciences, Hiroshima University, Hiroshima, Japan.
2Liver Center, Hiroshima University Hospital, Hiroshima, Japan.
*Corresponding Author: Tomokazu Kawaoka
Department of Gastroenterology, Graduate School of
Biomedical and Health Sciences, Hiroshima University,
Hiroshima, Japan.
Tel: +81-82-257-5192 & +81-82-257-5194;
Email: kawaokatomo@hiroshima-u.ac.jp
Abstract
Background and aim: Systemic therapy for unresectable Hepatocellular Carcinoma (u-HCC) has advanced in recent years, particularly immunotherapy. Atezolizumab plus bevacizumab has shown significant survival benefit in u-HCC, and recent AASLD guidelines recommend this regimen as a first-line option. On the other hand, drug withdrawal due to adverse events, especially those related to VEGF inhibition by bevacizumab, is often experienced in practice and remains an important issue. In this study, we investigated the prognostic impact of bevacizumab withdrawal in u-HCC patients treated with atezolizumab and bevacizumab.
Methods: Between October 2020 and February 2023, 169 patients who received atezolizumab plus bevacizumab for u-HCC at our institution consented to participate in the study. Patient data were collected retrospectively, including baseline characteristics, response rate, and prognosis.
Results: Of the 169 patients, 76 patients who continued atezolizumab plus bevacizumab for at least 6 months were included in the analysis; 40 patients experienced bevacizumab withdrawal. In efficacy analyses comparing those who withdrew bevacizumab at least once and those who never withdrew, no significant differences in response rate or survival were found. Additional studies on the timing of initial withdrawal and frequency of withdrawal of bevacizumab found no significant impact on the prognostic analysis.
Conclusions: No significant prognostic impact of bevacizumab withdrawal was observed in patients treated with atezolizumab plus bevacizumab. The results suggest that bevacizumab withdrawal may be acceptable for effective management of side effects.
Keywords: Hepatocellular carcinoma, Atezolizumab plus bevacizumab; Bevacizumab withdrawal; Radiological response; Overall survival; Progression-free survival.
Citation: Kawaoka T, Amioka K, Yamaoka K, Nakahara H, Yano S, et al. The Bevacizumab Skip in Atezolizumab plus Bevacizumab for Hepatocellular Carcinoma. SciBase Gastroenterol Hepatol. 2024; 1(1): 1005.
Introduction
Hepatocellular carcinoma develops against a background of chronic liver disease, such as viral hepatitis, fatty liver, and alcohol abuse. It has poor symptoms in the early stages and remains one of the leading causes of cancer-related deaths; in particular, unresectable Hepatocellular Carcinoma (u-HCC) is known to have a poor prognosis [1,2].
In systemic therapy for u-HCC, sorafenib was approved as the first Molecularly Targeted Agent (MTA) in 2007 based on two phase III trials demonstrating efficacy [3,4]. There were no effective new first-line systemic therapies for u-HCC for about 10 years after that, but lenvatinib was approved in 2018 based on the results of the REFLECT trial; since then, MTAs such as regorafenib, ramucirumab, and cabozantinib have been approved in Japan one after another, leading to an increase in the range of treatment options [5-8].
Furthermore, immunotherapy has developed rapidly in recent years. Immunocomplex therapy combining atezolizumab, a PD-L1 inhibitor, and bevacizumab, an inhibitor of Vascular Endothelial Growth Factor A (VEGF-A), was shown to have a statistically significant improvement in overall survival and progression-free survival compared to sorafenib in the IMbrave150 trial, leading to its approval in 2020 as a new first-line therapy for u-HCC [9]. More recently, the results of the HIMALAYA trial have led to the approval of durvalumab plus tremelimumab, which combines two immune checkpoint inhibitors (anti-programmed cell death ligand-1 antibody and anti-cytotoxic T-lymphocyte antigen 4 antibody), and durvalumab monotherapy as new immunotherapy regimens in Japan, making a total of 8 different regimens available [10].
Atezolizumab plus bevacizumab is one of the most effective regimens available for u-HCC. American Association for the Study of Liver Diseases (AASLD) Practice Guidance updated in 2023 recommends atezolizumab plus bevacizumab as the first choice regimen in patients with no autoimmune disease or history of liver transplantation who are unsuitable for immunotherapy and are not at high risk of gastrointestinal bleeding [11].
During treatment with atezolizumab plus bevacizumab, attention must be paid to both immune- and VEGF-inhibition-related adverse events, and early detection and intervention of adverse events are essential for good management and continuation of treatment. In particular, bevacizumab has caused adverse events such as worsening proteinuria and bleeding/thrombotic events, often requiring withdrawal of the drug, which has been a major issue in the continuation of atezolizumab plus bevacizumab treatment. On the other hand, there are few reports on the clinical impact of bevacizumab withdrawal, which remains to be clarified. Therefore, we investigated the prognostic effect of bevacizumab withdrawal in u-HCC patients treated with atezolizumab plus bevacizumab as systemic therapy.
Material and methods
Patients
Consent to participate in the study was obtained from 169 patients who received atezolizumab plus bevacizumab for u-HCC at our hospital between October 2020 and February 2023, and patient information including baseline characteristics, response rate, and prognosis was collected retrospectively. The diagnosis of HCC was made by pathology or by radiological diagnosis using dynamic contrast-enhanced Computed Tomography (CT) or Gadolinium Ethoxybenzyl Diethylenetriaminepentaacetic Acid (Gd-EOB-DTPA)-enhanced Magnetic Resonance Imaging (MRI). The radiological diagnosis was based on the characteristics of HCC with staining in the arterial phase followed by a washout pattern in the portal and equilibrium phases. With regard to the etiology of HCC, patients positive for Hepatitis B Virus Infection (HBV) surface antigen or Anti-Hepatitis C Virus infection (HCV) antibody were considered to have HCC due to viral etiology, while patients negative for HBV surface antigen and HCV anantibody were considered to have HCC due to non-viral etiology. The Child-Pugh classification and modified Albumin-Bilirubin (mALBI) grade were used to assess hepatic reserve. The mALBI grade was created to more closely evaluate patients with conventional Albumin-Bilirubin grade (ALBI) grade 2 and is graded on a 4-point scale (ALBI score ≤ - 2.60 was grade 1, - 2.60 < ALBI score ≤ - 2.27 was grade 2a, - 2.27 < ALBI score ≤ - 1.39 was grade 2b, and ALBI score > - 1.39 was grade 3) [12,13]. Tumor stage was assessed using the Barcelona Clinic Liver Cancer (BCLC) staging system and TNM classification [14,15].
Treatment with atezolizumab plus bevacizumab
Atezolizumab plus bevacizumab was administered according to the IMbrave150 protocol, with patients receiving 1200 mg of atezolizumab plus 15 mg/kg of bevacizumab intravenously every 3 weeks. Atezolizumab plus bevacizumab is recommended for Child-Pugh class A patients, but in this study, Child-Pugh B patients were also introduced to atezolizumab plus bevacizumab after sufficient informed consent to the patient by their physician. Adverse events were assessed using the Common Terminology Criteria for Adverse Events version 5.0 [16]. In the event of a drug-related adverse event, the drug was withdrawn or discontinued based on the Guide for Appropriate Use of atezolizumab Plus bevacizumab in Patients with Unresectable HCC developed for Japanese Physicians by Chugai Pharmaceutical Co Ltd, with the final decision made by the attending physician. For proteinuria, bevacizumab was withdrawn when the Urine Protein/Creatinine Ratio (UPCR) was ≥2.0 and resumed when the UPCR was < 2.0. When performing the invasive procedure, bevacizumab was withdrawn for 3-6 weeks each before and after the procedure, depending on the invasiveness of the procedure. Patients continued treatment with atezolizumab plus bevacizumab until death or one of the following treatment discontinuation criteria was met: disease progression following treatment, adverse events requiring discontinuation of treatment, deterioration of Eastern Cooperative Oncology Group performance status (ECOG) PS to 4, worsening of hepatic reserves, or withdrawal of consent to participate in this study.
Assessment of response to atezolizumab plus bevacizumab
Radiological response was assessed by CT or MRI after the first 6 weeks following the start of atezolizumab plus bevacizumab, and every 9 weeks thereafter. Radiological treatment response was assessed using the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1 and the modified Response Evaluation Criteria in Solid Tumors (mRECIST) guidelines, and Overall Response Rate (ORR) and disease control rate (DCR) were assessed according to these guidelines [17,18]. Overall Survival (OS) was defined as the time from the start of atezolizumab plus bevacizumab until death from any cause, with a censoring date of the last follow-up date for patients who were alive. Progression-Free Survival (PFS) was defined as the time from the start of atezolizumab plus bevacizumab until radiological progression due to mRECIST or death from any cause. For patients alive without radiological progression, the date of the last radiological assessment or switch to the next treatment was the censoring date.
Definition of relative dose intensity
To assess the impact of bevacizumab withdrawal, this study defined the ratio of the number of cycles of bevacizumab to atezolizumab as the Relative Dose Intensity (RDI). RDI equals the number of cycles of bevacizumab divided by the number of cycles of atezolizumab, e.g., RDI=1 in the group that never skipped bevacizumab.
Statistical analysis
Statistical analysis was performed using the Kaplan-Meier method, log-rank test, chi-square test, Fisher’s exact test, and Mann-Whitney U-test. A significant difference was considered to exist if the p-value was less than 0.05. All statistical analyses were performed using IBM SPSS software (v.22.0.0).
Results
Clinical characteristics of participating patients
Of the 169 patients who consented to participate in this study, those who had received atezolizumab plus bevacizumab for at least 6 months were included to minimize immortal time bias. As a result, 76 patients were included in this analysis, excluding 23 patients who were ongoing but less than 6 months into therapy and 70 patients who discontinued within 6 months after starting therapy. Of the 76 patients included, 40 required withdrawal of bevacizumab during the course of therapy. The reasons for withdrawal of bevacizumab were proteinuria in 23 patients, bleeding and thrombotic events in 8 patients, invasive procedures in 6 patients, and worsening of general condition in 3 patients. To examine the effect of bevacizumab withdrawal, patients were divided into two groups: those who had never skipped bevacizumab (Bev never skipped group, n=36) and those who skipped bevacizumab at least once (Bev skipped group, n=40) (Figure 1).
Patient clinical characteristics are shown in Table 1. In the Bev never skipped group and the Bev skipped group, the median age was 70 and 73 years, male/female 32/4 and 32/8, performance status 0/1 33/3 and 39/1, and the cause of HCC was viral/non-viral 17/19, 16/24 patients, respectively. Child-Pugh grade at the start of atezolizumab plus bevacizumab was A/B 32/4 and 37/3, mALBI grade was 1-2a/2b 23/13 and 30/10, and BCLC stage was A-B/C 17/19 and 21/19, respectively. Atezolizumab plus bevacizumab was introduced as first-line/≥second-line in 25/11 and 26/14 patients, respectively. There were no clear differences in any of the background factors between the Bev never skipped group and the Bev skipped group.
Efficacy of atezolizumab plus bevacizumab
We compared the efficacy between the groups with and without bevacizumab withdrawal. In the bevacizumab never skipped group and bevacizumab skipped group, the ORR was 52.8%/50.0% and the DCR was 94.4%/95.0% by RECIST evaluation, and the ORR was 66.7%/70.0% and the DCR was 91.7%/95.0% by mRECIST evaluation, respectively, none of which showed significant differences (p-values; RECIST (ORR: 0.809, DCR: 0.914), mRECIST (ORR: 0.755, DCR: 0.558) (Table 2). The OS was 22.1 months/not reached, and the PFS by mRECIST evaluation was 11.7 months/12.2 months in the bevacizumab never skipped group and the bevacizumab skipped group, respectively, with no significant differences between the two groups (p-values; OS: 0.684, PFS: 0.369) (Figure 2).
Relative dose intensity of bevacizumabWe continued our efficacy analysis focusing on dosing status to examine the extent to which bevacizumab withdrawal is acceptable. The status of bevacizumab dosing by RDI is shown in Figure 3a. Of the 40 patients in the bevacizumab skipped group, 12 had RDI values of 0.9-1.0 and 10 had RDI values of 0.8-0.9, with a wide range of other values.
We compared efficacy in the following four groups by RDI (1/0.9-1.0/0.6-0.9/< 0.6). The results are shown in Table 3 and Figure 3. The ORR and DCR in the RECIST evaluation were 52.8%/50.0%/41.2%/63.6% and 94.4%/100.0%/94.1%/90.9%, respectively, while the ORR and DCR in the mRECIST evaluation were 66.7%/58.3%/70.6%/81.8% and 91.7%/100.0%/94 .1%/90.9%, with no significant differences between each other (p-values; RECIST (ORR: 0.727, DCR: 0.805), mRECIST (ORR: 0.707, DCR: 0.845). The OS was 22.1 months/not reached/16.9 months/not reached, and the PFS by mRECIST evaluation was 11.7 months/12.4 months/15.9 months/10.5 months, none of which were significantly different from each other (p-value; OS: 0.571, PFS: 0.738).
The timing of the first withdrawal of bevacizumab
Finally, we examined the impact of efficacy as affected by the timing of the first withdrawal of bevacizumab. The cycle timing of the first withdrawal of bevacizumab is shown in Figure 4a. There was a wide range in the cycle timing for the first withdrawal of bevacizumab, from early to late.
We compared efficacy by dividing the cycle timing of the first withdrawal of bevacizumab into four groups: 2-4th/5th-9th/10th or more/never skipped. The results are shown in Table 4 and Figure 4. The ORR and DCR in the RECIST evaluation were 40.0%/47.1%/61.5%/52.8% and 90.0%/100.0%/92.3%/94.4%, respectively, while the ORR and DCR in the mRECIST evaluation were 70.0%/70.6%/69.2%/66.7% and 90.0%/100.0%/92.3%/91.7%, with no significant differences (p-values; RECIST (ORR: 0.765, DCR: 0.574), mRECIST (ORR: 1.000, DCR: 0.606). The OS was not reached/21.0 months/not reached/22.1 months, and the PFS by mRECIST evaluation was 10.0 months/12.0 months/15.9 months/11.7 months, respectively, with no significant differences (p-value; OS: 0.873, PFS: 0.661).
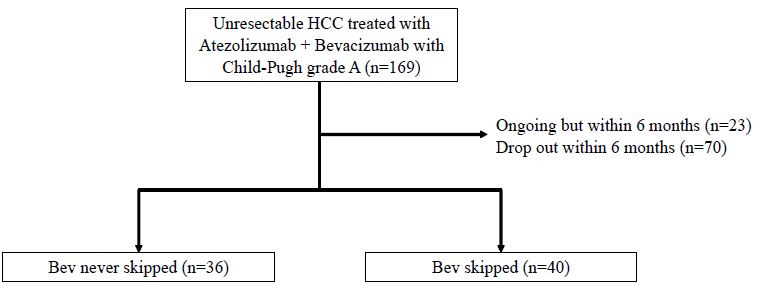
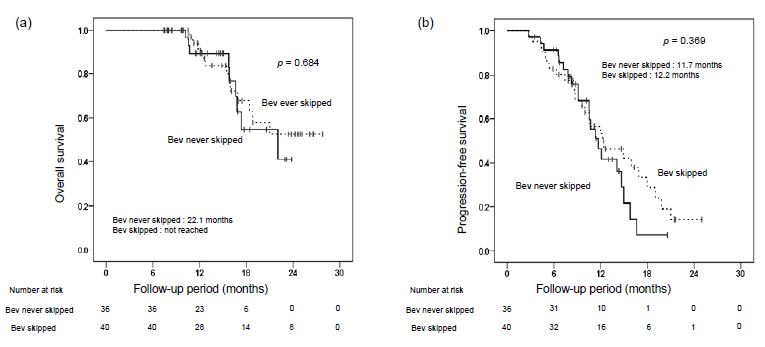
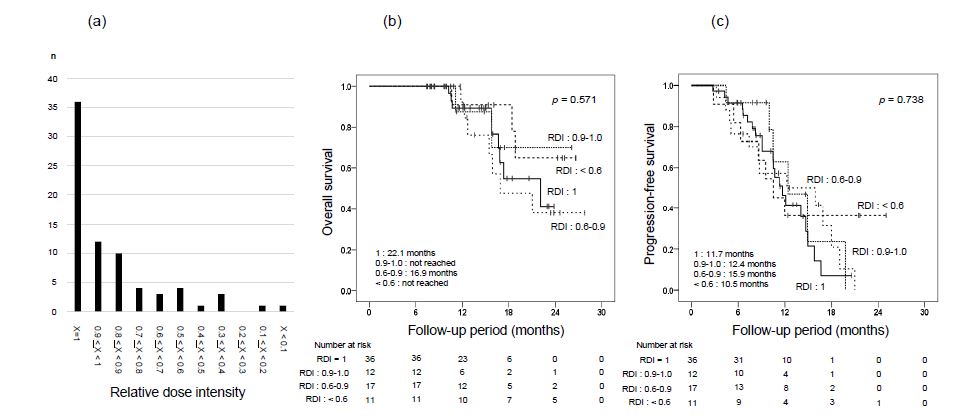
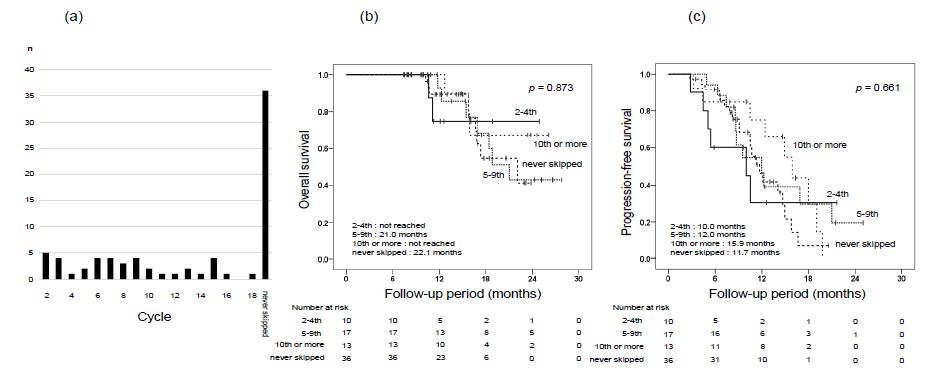
Table 1: Clinical characteristics at initiation of Atezo+Bev (n=76).
| Bev neverskipped (n=36) | Bev skipped (n=40) | p value | |
|---|---|---|---|
| Age (years) * | 70 (55-90) | 73 (59-89) | 0.131 |
| Gender (males/females), n | 32/4 | 32/8 | 0.289 |
| Performance status(0/1), n | 33/3 | 39/1 | 0.256 |
| Etiology (viral/non-viral), n | 17/19 | 16/24 | 0.526 |
| Child-Pugh score(A/B), n | 32/4 | 37/3 | 0.587 |
| mALBI grade(1-2a/2b), n | 23/13 | 30/10 | 0.292 |
| Relative tumorvolume (<50%/>50%), n | 35/1 | 38/2 | 0.619 |
| Size of liver tumor(mm) * | 26.0 (0.0-130.0) | 36.5 (0.0-130.0) | 0.369 |
| Number of intrahepatic tumor(<3/>4), n | 17/19 | 20/20 | 0.809 |
| MVI (absent/present), n | 27/9 | 34/6 | 0.274 |
| Extrahepatic metastasis (absent/present), n | 23/13 | 22/18 | 0.431 |
| TNM stage(II-III/IVa-IVb), n | 20/16 | 22/18 | 0.961 |
| BCLC stage(A-B/C), n | 17/19 | 21/19 | 0.646 |
| AFP (ng/ml) * | 8.0 (1.0-8000.0) | 18.6 (1.5-34200.0) | 0.470 |
| DCP (mAU/ml) * | 181 (26-60910) | 225 (17-108710) | 0.632 |
| Line of Atezo+Bev (1st/2nd or later) | 25/11 | 26/14 | 0.681 |
Atezo+Bev: Atezolizumab, Bevacizumab; mALBI: Modified Albumin-Bilirubin; MVI: Macroscopic Vascular Invasion; BCLC: Barcelona Clinic Liver Cancer; AFP: Alpha-fetoprotein; DCP: Des-γ-carboxy prothrombin.
Table 2: Radiological best responses to Atezo+Bev in the group that never skipped Bev versus the group that skipped Bev one or more times.
| RECIST % (n) | mRECIST % (n) | |||||
|---|---|---|---|---|---|---|
| Bevnever skipped | Bevever skipped | p value | Bevnever skipped | Bevever skipped | p value | |
| n=36 | n=40 | n=36 | n=40 | |||
| CR | 5.6 (2) | 2.5 (1) | 11.1 (4) | 10.0 (4) | ||
| PR | 47.2 (17) | 47.5 (19) | 55.6 (20) | 60.0 (24) | ||
| SD | 41.7 (15) | 45.0 (18) | 25.0 (9) | 25.0 (10) | ||
| PD | 5.6 (2) | 5.0 (2) | 8.3 (3) | 5.0 (2) | ||
| ORR | 52.8 (19) | 50.0 (20) | 0.809 | 66.7 (24) | 70.0 (28) | 0.775 |
| DCR | 94.4 (34) | 95.0 (38) | 0.914 | 91.7 (33) | 95.0 (38) | 0.558 |
RECIST: Response Evaluation Criteria in Solid Tumors; mRECIST: Modified Response Evaluation Criteria in Solid Tumors; CR: Complete Response; PR: Partial Response; SD: Stable Disease; PD: Progressive Disease; ORR: Overall Response Rate; DCR: Disease Control Rate.
Table 3: Radiological responses to Atezo+Bev according to RDI of Bev.
| RECIST % (n) | mRECIST % (n) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 n=36 | 0.9-1.0 n=12 | 0.6-0.9 n=17 | <0.6 n=11 | p value | 1 n=36 | 0.9-1.0 n=12 | 0.6-0.9 n=17 | <0.6 n=11 | p value | |
| CR | 5.6 (2) | (0) | 5.9 (1) | (0) | 11.1 (4) | 8.3 (1) | 11.8 (2) | 9.1 (1) | ||
| PR | 47.2 (17) | 50.0 (6) | 35.3 (6) | 63.6 (7) | 55.6 (20) | 50.0 (6) | 58.8 (10) | 72.7 (8) | ||
| SD | 41.7 (15) | 50.0 (6) | 52.9 (9) | 27.3 (3) | 25.0 (9) | 41.7 (5) | 23.5 (4) | 9.1 (1) | ||
| PD | 5.6 (2) | (0) | 5.9 (1) | 9.1 (1) | 8.3 (3) | (0) | 5.9 (1) | 9.1 (1) | ||
| ORR | 52.8 (19) | 50.0 (6) | 41.2 (7) | 63.6 (7) | 0.727 | 66.7 (24) | 58.3 (7) | 70.6 (12) | 81.8 (9) | 0.707 |
| DCR | 94.4 (34) | 100.0 (12) | 94.1 (16) | 90.9 (10) | 0.805 | 91.7 (33) | 100.0 (12) | 94.1 (16) | 90.9 (10) | 0.845 |
RECIST: Response Evaluation Criteria in Solid Tumors; mRECIST: Modified Response Evaluation Criteria in Solid Tumors; CR: Complete Response; PR: Partial Response; SD: Stable Disease; PD: Progressive Disease; ORR: Overall Response Rate; DCR: Disease Control Rate.
Table 4: Radiological responses to Atezo+Bev according to the cycle of the first withdrawal of Bev.
| RECIST % (n) | mRECIST % (n) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 2-4th n=10 | 5-9th n=17 | 10th or more n=13 | never skippedn=36 | p value | 2-4th n=10 | 5-9th n=17 | 10th or more n=13 | never skippedn=36 | p value | |
| CR | (0) | 5.9 (1) | (0) | 5.6 (2) | (0) | 11.8 (2) | 15.4 (2) | 11.1 (4) | ||
| PR | 40.0 (4) | 41.2 (7) | 61.5 (8) | 47.2 (17) | 70.0 (7) | 58.8 (10) | 53.8 (7) | 55.6 (20) | ||
| SD | 50.0 (5) | 52.9 (9) | 30.8 (4) | 41.7 (15) | 20.0 (2) | 29.4 (5) | 23.1 (3) | 25.0 (9) | ||
| PD | 10.0 (1) | (0) | 7.7 (1) | 5.6 (2) | 10.0 (1) | (0) | 7.7 (1) | 8.3 (3) | ||
| ORR | 40.0 (4) | 47.1 (8) | 61.5 (8) | 52.8 (19) | 0.765 | 70.0 (7) | 70.6 (12) | 69.2 (9) | 66.7 (24) | 1 |
| DCR | 90.0 (9) | 100.0 (17) | 92.3 (12) | 94.4 (34) | 0.574 | 90.0 (9) | 100.0 (17) | 92.3 (12) | 91.7 (33) | 0.606 |
RECIST, Response Evaluation Criteria in Solid Tumors; mRECIST: Modified Response Evaluation Criteria in Solid Tumors; CR: Complete Response; PR: Partial Response; SD: Stable Disease; PD: Progressive Disease; ORR: Overall Response Rate; DCR: Disease Control Rate.
Discussion
In this study, we evaluated the prognostic impact of bevacizumab withdrawal in patients with u-HCC treated with atezolizumab plus bevacizumab at our institution. Of the 76 patients, 40 required at least one bevacizumab withdrawal during the course of treatment.
There were no significant differences in patient background at the time of introduction of atezolizumab plus bevacizumab between the two groups (“Bev never skipped group” and “Bev skipped group”). Results for radiological best response were similar between the two groups for both mRECIST and RECIST evaluation. There were no significant differences in OS and PFS between the two groups. No prognostic impact of bevacizumab withdrawal was observed in this study.
Atezolizumab plus bevacizumab has shown superior clinical outcomes compared to sorafenib and is now established as the standard systemic therapy for u-HCC. In fact, according to the BCLC staging system in the AASLD practice guidance updated in 2023 and the Clinical Practice Guidelines for Hepatocellular Carcinoma in Japan updated in May 2023, two regimens, durvalumab plus tremelimumab and atezolizumab plus bevacizumab are recommended when immunotherapy is indicated [19,20]. Atezolizumab plus bevacizumab is a combination immunotherapy that includes atezolizumab, a PD-L1 inhibitor, and bevacizumab, which inhibits VEGF-A, and can achieve better efficacy in combination with an angiogenesis inhibitor than with an immune checkpoint inhibitor alone. In Arm F of the GO30140 trial comparing atezolizumab plus bevacizumab to atezolizumab alone, the primary endpoint of PFS was 5.6 months in the atezolizumab plus bevacizumab arm and 3.4 months in the atezolizumab alone arm, with clear improvement in efficacy with the combination of bevacizumab [21].
On the other hand, attention must be paid to immune-related adverse events attributable to atezolizumab and adverse events attributable to bevacizumab, particularly in real-world clinical practice, where bevacizumab withdrawal is frequently necessary.
Bevacizumab withdrawal is an important clinical issue, but its prognostic impact has been reported in very few studies. The two studies in patients enrolled in the IMbrave150 and GO30140 trials reported no prognostic effect of bevacizumab withdrawal in HCC patients treated with atezolizumab plus bevacizumab for more than 6 months [22,23]. Although there have been several studies of disease progression after bevacizumab discontinuation in other types of carcinomas, we did not find any reports examining the prognostic impact of bevacizumab withdrawal [24-27]. Bevacizumab withdrawal criteria for proteinuria vary by carcinoma, and HCC patients tend to be treated with a stricter UPCR 2.0 withdrawal regimen in practice than other carcinomas, which may be one reason why bevacizumab withdrawal is a clinical problem in the practice of HCC.
We analyzed the question of how much of a withdrawal of bevacizumab is acceptable, focusing on the ratio of the number of cycles of bevacizumab to atezolizumab (RDI). The RDI varied, and a comparison of the RDIs in the four groups showed no clear difference in prognosis. Although combination use of bevacizumab is important, the results suggest that the proportion of bevacizumab administered after initiation of atezolizumab plus bevacizumab may not have a significant impact on prognosis. In the cancer immune cycle, bevacizumab has a variety of roles, including not only direct antitumor effects by inhibiting angiogenesis, but also promoting T cell priming, facilitating cytotoxic T cell infiltration into the tumor by normalizing tumor vascular architecture, and releasing immunosuppression of the tumor microenvironment [28-31]. The results of this study may be influenced by the effects of bevacizumab on the tumor microenvironment, primarily by promoting T cell priming.
In addition, since bevacizumab withdrawal is often required early after initiation, we focused our analysis on the prognostic impact of the timing of the first bevacizumab withdrawal. In this study, the timing of the first bevacizumab withdrawal in the Bev skipped group varied from early to late cycles. A comparison of prognosis among the four groups divided by the time of first withdrawal, including the Bev never skipped group, showed no clear difference. These results suggest that bevacizumab withdrawal may be acceptable even early after initiation.
In the updated analysis of the IMbrave150 trial, proteinuria and hypertension were the most frequent adverse events attributed to bevacizumab in about 30% of patients, and potentially serious events such as bleeding and thrombosis were observed in a certain proportion of patients [32]. In particular, proteinuria is often the cause of bevacizumab withdrawal because it triggers decreased hepatic reserve and renal failure, thus the management of proteinuria is an important issue in the management of bevacizumab. In this study, a UPCR of 2.0 or higher was used as an indicator of withdrawal according to the Guide for Appropriate Use of Atezolizumab Plus Bevacizumab in Patients with Unresectable HCC developed for Japanese Physicians by Chugai Pharmaceutical Co Ltd, and 23 of the 76 patients overall required withdrawal of bevacizumab due to proteinuria, which was the most common reason for withdrawal. Takaki et al. reported a significantly better OS in patients with proteinuria compared to those without proteinuria in their study of atezolizumab plus bevacizumab for u-HCC [33]. Similarly, in this study, the OS was significantly better in patients who experienced a worsening grade of proteinuria after initiation than in those without. In addition, a significantly better ORR was observed in patients with a worsening grade of proteinuria than in those without in the best response evaluated by mRECIST. These results suggest that the presence of proteinuria may reflect a positive response to bevacizumab. One reason why bevacizumab withdrawal did not affect prognosis in this study may have been the association between the appearance of proteinuria, which accounted for about half of the reasons for withdrawal, and prognosis. Management is very important for the effective continuation of atezolizumab plus bevacizumab, which is expected to have favorable efficacy and maintain quality of life in systemic therapy for HCC. The results of this study, using real clinical data, indicate that withdrawal of bevacizumab, especially for proteinuria, may be acceptable in terms of prognosis.
There are several limitations to this study. First, it was a single-center, retrospective study. The observation period and sample size were limited. Second, 9% (7 patients) were initiated with Child-Pugh grade B, and 33% (25 patients) had a history of systemic therapy. Third, the impact of bevacizumab withdrawal on detailed response after withdrawal was not analyzed. Therefore, further studies with larger, prospective studies and adequate observation periods are needed.
In conclusion, this study did not identify any apparent prognostic impact of bevacizumab withdrawal during atezolizumab plus bevacizumab treatment, suggesting that bevacizumab withdrawal may be acceptable.
Abbreviations: AASLD: American Association for the Study of Liver Diseases; ALBI: Albumin-Bilirubin; BCLC: Barcelona Clinic Liver Cancer; CT: Computed Tomography; ECOG: Eastern Cooperative Oncology Group; DCR: Disease Control Rate; Gd-EOB-DTPA: Gadolinium Ethoxybenzyl Diethylenetriaminepentaacetic Acid; HBV: Hepatitis B Virus; HCV: Hepatitis C Virus; mALBI: modified Albumin-Bilirubin; MRI: Magnetic Resonance Imaging; mRECIST: modified Response Evaluation Criteria in Solid Tumors; MTA: Molecularly Targeted Agent; OS: Overall Survival; PFS: Progression Free Survival; RDI: Relative Dose Intensity; RECIST: Response Evaluation Criteria in Solid Tumors; ORR: Overall Response Rate; u-HCC: unresectable Hepatocellular Carcinoma; UPCR: Urine Protein/Creatinine Ratio; VEGF-A: Vascular Endothelial Growth Factor A.
Declarations
Conflict of interest disclosure: The authors have no conflicts of interest to disclose.
Funding statement: Not applicable.
Author’s contributions: Kei Amioka and Tomokazu Kawaoka contributed to study conception, literature review, and writing the manuscript. Other authors contributed to the study design and data interpretation. All authors critically revised and commented on the manuscript, and approved the final version.
References
- Forner A, Reig M, Bruix J. Hepatocellular carcinoma. Lancet. 2018; 391: 1301-1314.
- Jemal A, Bray F, Center MM, Ferlay J, Ward E, et al. Global cancer statistics. CA Cancer J Clin. 2011; 61: 69-90.
- Llovet JM, Ricci S, Mazzaferro V, Hilgard P, Gane E, et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 2008; 359: 378-390.
- Cheng AL, Kang YK, Chen Z, Tsao CJ, Qin S, et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: A phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009; 10: 25-34.
- Kudo M, Finn RS, Qin S, Han KH, Ikeda K, Piscaglia F, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet. 2018; 391: 1163-1173.
- Bruix J, Qin S, Merle P, Granito A, Huang YH, et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2017; 389: 56-66.
- Zhu AX, Finn RS, Galle PR, Llovet JM, Kudo M. Ramucirumab in advanced hepatocellular carcinoma in REACH-2: The true value of alpha-fetoprotein. Lancet Oncol. 2019; 20: e191.
- Abou-Alfa GK, Meyer T, Cheng AL, El-Khoueiry AB, Rimassa L, et al. Cabozantinib in patients with advanced and progressing hepatocellular carcinoma. N Engl J Med. 2018; 379: 54-63.
- Finn RS, Qin S, Ikeda M, Galle PR, Ducreux M, et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med. 2020; 382: 1894-1905.
- Abou-Alfa GK, Lau G, Kudo M, Chan SL, Kelley RK, et al. Tremelimumab plus Durvalumab in Unresectable Hepatocellular Carcinoma. NEJM Evid. 2022; 1: EVIDoa2100070.
- Signal AG, Llovet JM, Yarchoan M, Mehta N, Heimbach JK, et al. AASLD Practice Guidance on prevention, diagnosis, and treatment of hepatocellular carcinoma. Hepatology. 2023; 78(6): 1922-1965.
- Johnson PJ, Berhane S, Kagebayashi C, Satomura S, Teng M, et al. Assessment of liver function in patients with hepatocellular carcinoma: A new evidence-based approach-the ALBI grade. J Clin Oncol. 2015; 33: 550-558.
- Hiraoka A, Kumada T, Tsuji, K, Takaguchi K, Itobayashi E, et al. Validation of modified ALBI grade for more detailed assessing hepatic function of hepatocellular carcinoma-Multicenter analysis. Liver Cancer. 2019; 8: 121-129.
- Forner A, Llovet JM, Bruix J. Hepatocellular carcinoma. Lancet. 2012; 379: 1245-1255.
- Bruix J, Reig M, Sherman M. Evidence-Based Diagnosis, Staging, and Treatment of Patients with Hepatocellular Carcinoma. Gastroenterology. 2016; 150: 835-853.
- Japan Clinical Oncology Group. Common Terminology Criteria for Adverse Events (CTCAE) version 5.0. 2022. http://www.jcog.jp/doctor/tool/ctcaev5.html.
- Schwartz LH, Seymour L, Litière S, Ford R, Gwyther S, et al. RECIST 1.1-Standardisation and disease-specific adaptations: Perspectives from the RECIST Working Group. Eur J Cancer. 2016; 62: 138-145.
- Lencioni R, Llovet JM. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis. 2010; 30: 52-60.
- Reig M, Forner A, Rimola J, Ferrer-Fabrega J, Burrel M, et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J Hepatol. 2022; 76(3): 681-693.
- https://www.jsh.or.jp/lib/files/medical/guidelines/jsh_guidlines/medical/guideline_jp_2021_cq39_algorithm.pdf.
- Lee MS, Ryoo BY, Hsu CH, Numata K, Stein S, et al. Atezolizumab with or without bevacizumab in unresectable hepatocellular carcinoma (GO30140): An open-label, multicentre, phase 1b study. Lancet Oncol. 2020; 21(6): 808-820.
- Shao YY, Feng YH, Yen CJ, Yang TS, Shen YC, et al. Bevacizumab and atezolizumab as first-line therapy for advanced hepatocellular carcinoma: A Taiwanese subgroup analysis on efficacy and safety. J Formos Med Assoc. 2022; 121(12): 2430-2437.
- Kudo M, Tsuchiya K, Shao YY, Finn RS, Galle PR, et al. IMbrave150: Exploratory analysis to examine the association between bevacizumab (bev) ever being skipped and bev never being skipped in patients with unresectable Hepatocellular Carcinoma (HCC) treated with atezolizumab (atezo) + bev in a global Phase 3 study. ASCO-GI. 2023; 538.
- Takamatsu S, Nakai H, Yamaguchi K, Hamanishi J, Mandai M, et al. Time-Dependent Changes in Risk of Progression During Use of Bevacizumab for Ovarian Cancer. JAMA Netw Open. 2023; 6(8): e2326834.
- Kim BS, Kim SK, Choi SH, Lee SH, Seol HJ, et al. Prognostic implication of progression pattern after anti-VEGF bevacizumab treatment for recurrent malignant gliomas. J Neurooncol. 2015; 124(1): 101-10.
- Anderson MD, Hamza MA, Hess KR, Puduvalli VK. Implications of bevacizumab discontinuation in adults with recurrent glioblastoma. Neuro Oncol. 2014; 16(6): 823-8.
- Zhu LM, Zhao YZ, Ju HX, Liu LY, Chen L, et al. Efficacy and safety of bevacizumab in Chinese patients with metastatic colorectal cancer. Asian Pac J Cancer Prev. 2014; 15(16): 6559-64.
- Facciabene A, Peng X, Hagemann IS, Balint K, Barchetti A, et al. Tumour hypoxia promotes tolerance and angiogenesis via CCL28 and T(reg) cells. Nature. 2011; 475(7355): 226-230.
- Chen DS, Mellman I. Oncology meets immunology: the cancer-immunity cycle. Immunity. 2013; 39(1): 1-10.
- Hodi FS, Lawrence D, Lezcano C, Wu X, Zhou J, et al. Bevacizumab plus ipilimumab in patients with metastatic melanoma. Cancer Immunol Res. 2014; 2(7): 632-642.
- Wallin JJ, Bendell JC, Funke R, Sznol M, Korski K, et al. Atezolizumab in combination with bevacizumab enhances antigen-specific T-cell migration in metastatic renal cell carcinoma. Nat Commun. 2016; 7: 12624.
- Cheng AL, Qin S, Ikeda M, Galle PR, Ducreux M, et al. Updated efficacy and safety data from IMbrave150: Atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. J Hepatol. 2022; 76(4): 862-873.
- Takaki S, Kurosaki M, Mori N, Tsuji K, Ochi H, et al. Effects on survival of the adverse event of atezolizumab plus bevacizumab for hepatocellular carcinoma: A multicenter study by the Japan Red Cross Liver Study Group. Invest New Drugs. 2023; 41(2): 340-349.