
SciBase Journals
SciBase Gastroenterology and Hepatology
- Article Type: Research Article
- Volume 1, Issue 2
- Received: Sep 26, 2024
- Accepted: Oct 31, 2024
- Published Online: Nov 07, 2024
The Bedside Index for Severity in Acute Pancreatitis Score Combines with the Modified Computed Tomography Severity Index to Early Predict the Severity of Acute Pancreatitis
Wenyun Zhu1#; Yang Liu2#; Fangren Sun3; Huabin Zhong1; Yunpeng Yuan4; Tingting Gong5*
1Department of Gastroenterology, Ruijin People’s Hospital of Jiangxi province, Ruiijn, China.
2Department of Endocrinology, China Resources and WISCO General Hospital, Wuhanm China.
4Department of Neurosurgery, Baoshan Campus, Shuguang Hospital, Shanghai University of Traditional Chinese Medicine, Shanghai,
China.
5Department of Gastroenterology, Ruijin Hospital, Shanghai Jiaotong University, Shanghai, China.
#Wenyun Zhu and Yang Liu contributed equally to this paper.
*Corresponding Author: Tingting Gong
Department of Gastroenterology, Ruijin Hospital, Shanghai
Jiaotong University, Shanghai, China.
Email: 3414119@zju.edu.cn
Abstract
Background and objectives: To assess the significance of early prognostication using the Bedside Index for Severity in Acute Pancreatitis (BISAP) score combined with the Modified Computed Tomography Severity Index (MCTSI) in determining the severity of acute pancreatitis.
Materials and methods: 153 patients with acute pancreatitis were retrospectively screened from June 2020 to May 2021 at Ruijin Hospital. A total of 141 patients were included in this study and were divided into two groups. The Severe Acute Pancreatitis (SAP) group consisted of 88 cases (62.4%), while the Mild Acute Pancreatitis and Moderately Severe Acute Pancreatitis (MAP/MSAP) group consisted of 53 cases (37.6%). BISAP scores and MCTSI were assessed within 24 hours after admission. The specific methods employed included analyzing patients’ characteristics, constructing Receiver Operating Characteristic (ROC) curves, and discussing the relationship between BISAP scores, MCTSI, and their predictive value for acute pancreatitis severity.
Results: The more severe the acute pancreatitis was, the higher the scores of BISAP and MCTSI increased (p< 0.05). There was a positive correlation between the BISAP score and MCTSI (r=0.492, p< 0.05). The Area Under the ROC Curve (AUC) for the severity of acute pancreatitis was 0.771 for the BISAP score, 0.790 for the MCTSI, and 0.840 for the combined B-M (BISAP combined with MCTSI). These results also showed a statistically significant difference (p< 0.01).
Conclusions: The BISAP score and MCTSI demonstrated strong evaluative capabilities in assessing the severity of acute pancreatitis individually, and their combined use is even more significant.
Keywords: Bedside index for severity in acute pancreatitis (BISAP); Modified CT severity index (MCTSI); Prediction; Acute pancreatitis.
Citation: Zhu W, Liu Y, Sun F, Zhong H, Gong T, et al. The Bedside Index for Severity in Acute Pancreatitis Score Combines with the Modified Computed Tomography Severity Index to Early Predict the Severity of Acute Pancreatitis. SciBase Gastroenterol Hepatol. 2024; 1(2): 1007.
Introduction
Acute pancreatitis is a condition caused by the activation of tryptase due to various factors. Its primary symptom is local inflammation of the pancreas, often accompanied by dysfunction of one or multiple organs [1]. Acute pancreatitis is a self-limiting disease, but approximately 20-30% of patient’s progress to severe acute pancreatitis, which carries a high mortality rate of up to 10% if early and proper treatment is not administered [2]. Therefore, early assessment of the severity of acute pancreatitis is crucial for promptly monitoring patients’ condition, providing appropriate treatment, and reducing hospital stays.
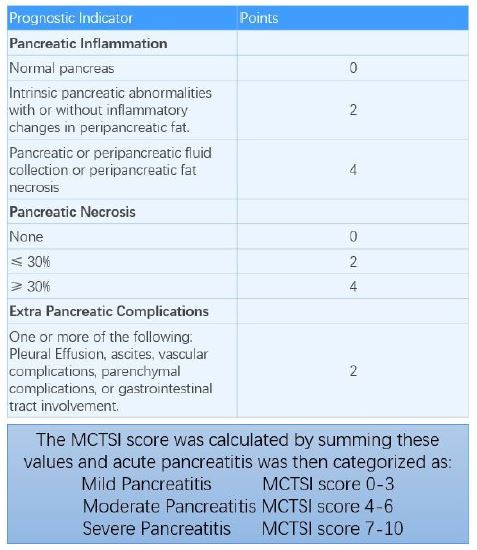
Currently, several scoring systems are used in hospitals to grade the severity of acute pancreatitis, such as the Bedside Index for Severity in Acute Pancreatitis (BISAP) score, modified Computed Tomography Severity Index (MCTSI, Figure 1), Acute Physiology and Chronic Health Evaluation (APACHE) II score, and Ranson’s score, among others [3,4]. However, some of these scoring systems are complex and require extensive clinical data, limiting their use in clinical practice. Studies have shown that MCTSI is a straightforward scoring system, while BISAP is easier to use, and both have high value in assessing the severity of acute pancreatitis [5,6]. However, the combined use of BISAP and MCTSI has not been reported yet. Therefore, it is necessary to conduct comprehensive, repeated, and systematic analysis of clinical indicators such as age, blood urea nitrogen, temperature, blood white cell count, impaired mental status, and imaging evidence of pleural effusion to accurately assess the severity of acute pancreatitis. In this study, we aim to evaluate the early prognostic value and correlations between BISAP scores combined with modified CTSI and each scoring system individually in determining the severity of acute pancreatitis.
Materials and methods
Materials
Data from 153 cases of acute pancreatitis were collected retrospectively over a one-year period from June 2020 to May 2021 at Ruijin Hospital. Twelve cases were excluded for various reasons, including being under the age of 18, receiving treatment for pancreatitis at another hospital, having complications with malignant tumors or other diseases. This resulted in a total of 141 included cases. Among them, 88 patients were male (62.4%), while the remaining 53 were female (37.6%). The average age was 49.65±15.92 years, with an age range of 18 to 88 years. The inclusion criteria were as follows: 1) Diagnosis and grading of acute pancreatitis aligned with guidelines [7]; 2) Patients presented to the hospital within 24 hours of symptom onset; 3) Obtained Computed Tomography (CT) scans and related laboratory tests within the first 24 hours of hospital admission, with complete relevant information. The exclusion criteria were: 1) Being under the age of 18; 2) previously treated for pancreatitis at another hospital; 3) Presence of underlying diseases such as chronic pancreatitis, malignant tumors, or severe diseases of other organs. The enrolled patients with acute pancreatitis were divided into two groups according to the guidelines: 88 cases in the Severe Acute Pancreatitis (SAP) group and 53 cases in the Mild Acute Pancreatitis and Moderately Severe Acute Pancreatitis (MAP/MSAP) group.
Methods
The following information was collected for the acute pancreatitis patients: gender, age, triglyceride levels, blood urea nitrogen levels, impaired mental status, evidence of systemic inflammatory response syndrome, and imaging evidence of pleural effusion. BISAP scores and MCTSI scores were calculated for each patient with acute pancreatitis.
Statistical analysis
Statistical analysis was conducted using SPSS 26.0. The values are presented as mean ± Standard Deviation (SD). Independent samples t-tests were used to compare two sets of measurement data, while chi-square tests were used for comparison of counting data. Spearman correlation analysis was employed to assess the correlation between the two variables. Receiver-Operating Characteristic (ROC) curves were constructed for the three scoring systems: BISAP score, MCTSI score, and B-M score, to measure the predictive accuracy of each system by calculating the Area under the Curve (AUC). A p-value< 0.05 was considered statistically significant.
Results
Patient characteristics (age, sex, and etiological factors) were analyzed between the two groups (MAP/MSAP and SAP). The comparison results showed no statistically significant difference between these two groups (p>0.05, (Table 1)).
Table 1: Patient characteristic at baseline.
| Characteristic | MAP/MSAP | SAP | P value | |
|---|---|---|---|---|
| Gender | Female | 18 | 35 | 0.490 |
| Male | 35 | 53 | ||
| Age | 49.98±15.020 | 49.35±15.971 | 0.059 | |
| Etiology | Hypertriglyceridemia | 15 | 34 | 0.129 |
| Gallstone | 14 | 27 | ||
| Surgery-related | 2 | 0 | ||
| Othercauses | 22 | 27 | ||
Comparison of the predictive value for acute pancreatitis severity between BISAP score and MCTSI, and exploration of their interrelationships. Compared to the MAP/MSAP group, the SAP group exhibited significantly higher BISAP scores (2.17±1.02 vs. 1.06±0.99 in the MAP/MSAP group, p< 0.0001, (Table 2)). Similarly, the SAP group had significantly higher MCTSI scores compared to the MAP/MSAP group (5.74±1.50 vs. 3.81±1.68 in the MAP/MSAP group, p< 0.0001, (Table 2)). The results of the Levin test for homogeneity of variance were as follows: BISAP score, F=0.060, p=0.897>0.05, and MCTSI, F=0.607, p=0.437>0.05, (Table 3). The data exhibited homogeneity in variance. The results comparing BISAP scores between the SAP group and the MAP/MSAP group indicated a significant difference (Sig. (two-tailed)=.000, (Table 4)). Additionally, the results comparing MCTSI scores between the SAP group and the MAP/MSAP group also indicated a significant difference (Sig. (two-tailed) = .000, (Table 4)). Moreover, correlation analysis between MCTSI and BISAP revealed a positive correlation (Pearson correlation=0.492, (Table 4)).
Table 2: Difference analysis.
| Index | AP groups | Patients number | Mean | Standard deviation(SD) | Mean standard error | Pvalue |
|---|---|---|---|---|---|---|
| BISAP | SAP | 88 | 2.17 | 1.020 | .109 | <0.0001 |
| MAP/MSAP | 53 | 1.06 | .989 | .136 | ||
| MCTSI | SAP | 88 | 5.75 | 1.510 | .161 | <0.0001 |
| MAP/MSAP | 53 | 3.81 | 1.676 | .230 |
Table 3: Independent sample test.
| Levin varianceequality test | Mean equality t-test | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| F | Significance | t | DF | Sig.(two-tailed) | Meandifference | Standarderror difference | Difference 95% confidence interval lowerlimit | Difference 95% confidence interval upperlimit | ||
| BISAP | Assumed equalvariance | .060 | .807 | 6.354 | 139 | .000 | 1.114 | .175 | .767 | 1.460 |
| No assumed equal variance | 6.403 | 112.388 | .000 | 1.114 | .174 | .769 | 1.458 | |||
| MCTSI | Assumed equalvariance | .607 | .437 | 7.081 | 139 | .000 | 1.939 | .274 | 1.397 | 2.480 |
| No assumed equal variance | 6.900 | 100.877 | .000 | 1.939 | .281 | 1.381 | 2.496 | |||
Table 4: Correlation analysis.
| BISAP | MCTSI | ||
|---|---|---|---|
| BISAP | Pearson correlation | 1 | .492** |
| Sig. (two-tailed) | .000 | ||
| Patients number | 141 | 141 | |
| MCTSI | Pearson correlation | .492** | 1 |
| Sig. (two-tailed) | .000 | ||
| Patients number | 141 | 141 |
ROC curve analysis of BISAP score, MCTSI score, and B-M combination in evaluating the severity of acute pancreatitis. Receiver-Operating Characteristic (ROC) curves were plotted for the three scoring systems: BISAP score, MCTSI score, and B-M score. The Area Under the ROC Curve (AUC) for these scoring systems was 0.771, 0.790, and 0.840, respectively (Figure 2). All three scores demonstrated good predictive value for severe acute pancreatitis, with the B-M score showing the highest performance.
ROC refer to receiver operating characteristic, BISAP refer to bedside index for severity in acute pancreatitis, MCTSI refer to modified computed tomography severity index.
Sensitivity (0.693, 0.761, and 0.898, (Table 5)) and specificity (0.774, 0.779, and 0.623, (Table 5)) of MCTSI, BISAP, and B-M scoring systems were evaluated for the early prediction of acute pancreatitis severity.
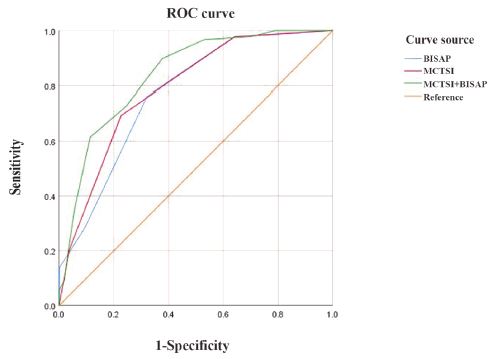
Table 5: Sensitivity and specificity analysis.
| Scoring systems | Youden's index | Sensitivity | Specificity | Score threshold |
|---|---|---|---|---|
| MCTSI | 0.467 | 0.693 | 0.774 | 5 |
| BISAP | 0.44 | 0.761 | 0.779 | 1.6 |
| B-M | 0.521 | 0.898 | 0.623 | 5.5 |
Discussion
The course and severity of acute pancreatitis were determined using the Atlanta classification revision of 2012 [8], which includes MAP, MSAP, and SAP. SAP is more commonly observed in late-stage pancreatitis and is considered a clinically critical and dangerous disease. Therefore, early evaluation and classification of disease severity are crucial for prognosis and management. Close monitoring, continuous evaluation, and rational intervention are necessary to improve the cure rate and survival rate.
Several studies [9-11] have been conducted on the value of early prediction of acute pancreatitis severity, such as using the BISAP score or Ranson score combined with D-dimer, serum albumin, C-reactive protein, serum procalcitonin, semi-lactose, agglutinin-9, IL-6 level, and other parameters for joint assessment. However, there is a lack of literature studying the combination of BISAP score and MCTSI to assess the early predictive value of acute pancreatitis severity. Thus, this study focuses on evaluating the value of BISAP scores and MCTSI in the early assessment of acute pancreatitis severity, as well as exploring the value of the B-M scoring system.
MCTSI and BISAP are commonly used clinical scoring systems [12,13] that offer certain advantages over other scoring criteria. The MCTSI score is a reliable system for early prediction of SAP severity. In the MCTSI scoring system, a total score of 3 or less indicates MAP, a score of 4, 5, or 6 indicates MSAP, and a score of ≥7 indicates SAP. CT has become one of the main diagnostic modalities for patients with acute pancreatitis, as it provides a comprehensive assessment of the abdominal cavity and thorax, with clearer visualization. The MCTSI scoring system is easy to calculate and can assess extra-parenchymal lesions, gastrointestinal tract or blood vessel invasion, pleural effusion, and ascites. The simplicity and repeatability of MCTSI scoring make it less subject to subjective influence by radiologists. MCTSI scores are positively correlated with risk factor scores for predicting complications and death in acute pancreatitis. Higher MCTSI scores are associated with increased morbidity and mortality. A study from China [14] ranked the early severity prediction accuracy of AP and found that MCTSI outperformed APACHE II and Ranson scoring systems, demonstrating the highest overall predictive power. This study confirms that MCTSI is a valuable scoring system for the early prediction of AP severity, with a sensitivity of 0.693 and specificity of 0.774.
The BISAP score, proposed in 2008 [5], consists of five observation items, and a score of ≥3 indicates SAP. BISAP scoring offers several advantages, including its simplicity with only five parameters, which are common clinical data and auxiliary examinations that are easy to obtain and calculate. Thus, early evaluation can be completed easily, facilitating its clinical application. Another study from China [11] demonstrated that BISAP is more predictive in patients with early-onset pancreatitis, with good positive and negative predictive values, and it is simple to use. Additionally, BISAP has superior value compared to the POP scoring system in predicting AP severity and assessing pancreatic necrosis. Other clinical studies [14,15] have shown that the AUC of the BISAP score for the severity of acute pancreatitis ranged from 0.711 to 0.856. In this study, the AUC of the BISAP score for the severity of acute pancreatitis was 0.771, consistent with the results of previous studies. Furthermore, the B-M (BISAP-MCTSI) scoring system demonstrated the highest AUC value (0.840), suggesting that the combination of the two systems has a higher value for early prediction of AP severity.
Clinical data collected from the SAP group and the MAP/MSAP group were compared. There were no significant differences in gender and age (p>0.05). However, significant differences (p< 0.01) were observed in BISAP scores and MCTSI scores between the two groups. BISAP scores and MCTSI scores are closely correlated with the severity of acute pancreatitis. Specifically, the more severe the acute pancreatitis, the higher the scores in both systems. Additionally, a positive correlation (r=0.492, p< 0.001) was found between the BISAP and MCTSI scoring systems. The predictive value of BISAP is better than MCTSI, and the B-M score has the highest evaluation value. All three scoring systems can be used as good parameters for the early prediction of AP severity. Moreover, the B-M scoring system shows a higher value in early prediction of AP severity.
Conclusion
summary, both the BISAP score and MCTSI are valuable scoring systems for predicting the condition of acute pancreatitis, with the B-M scoring system offering superior predictive value. However, this study has certain limitations as it is retrospective. The sample size is small, and the patients were enrolled from a single hospital in China. Prospective, large-scale, multicenter studies are still needed to further explore the early predictive value of BISAP scores, MCTSI, and other metrics.
Declarations
Author contributions: All of the authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by W.Z., Y.L., F.S. and H.Z. The first draft of the manuscript was written by W.Z. and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript. The revised manuscript was compiled by Y.P. and T.G.
Funding: This research received no external funding.
Informed consent statement: Informed consent was obtained from all subjects involved in the study.
Data availability statement: The data presented in this study are available on request from the corresponding authors.
Conflicts of interest: The authors declare no conflicts of interest.
References
- Mederos MA, Reber HA, Girgis MD. Acute Pancreatitis: A Review. JAMA. 2021; 325: 382-90.
- Leppaniemi A, Tolonen M, Tarasconi A, Segovia-Lohse H, Gamberini E, et al. 2019 WSES guidelines for the management of severe acute pancreatitis. World J Emerg Surg. 2019; 14: 27.
- Harshit Kumar A, Singh Griwan M. A comparison of APACHE II, BISAP, Ranson’s score and modified CTSI in predicting the severity of acute pancreatitis based on the 2012 revised Atlanta Classification. Gastroenterol Rep (Oxf). 2018; 6: 127-31.
- Chatterjee R, Parab N, Sajjan B, Nagar VS. Comparison of Acute Physiology and Chronic Health Evaluation II, Modified Computed Tomography Severity Index, and Bedside Index for Severity in Acute Pancreatitis Score in Predicting the Severity of Acute Pancreatitis. Indian J Crit Care Med. 2020; 24: 99-103.
- Singh VK, Wu BU, Bollen TL, Repas K, Maurer R, et al. A prospective evaluation of the bedside index for severity in acute pancreatitis score in assessing mortality and intermediate markers of severity in acute pancreatitis. Am J Gastroenterol. 2009; 104:966-71.
- Jain D, Bhaduri G, Jain P. Different Scoring Systems in Acute Alcoholic Pancreatitis: Which One to Follow? An Ongoing Dilema. Arq Gastroenterol. 2019; 56: 280-85.
- Working Group IAPAPAAPG. IAP/APA evidence-based guidelines for the management of acute pancreatitis. Pancreatology. 2013; 13: e1-15.
- Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, et al. Classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013; 62: 102-11.
- Woo SM, Noh MH, Kim BG, Hsing CT, Han JS, et al. Comparison of serum procalcitonin with Ranson, APACHE-II, Glasgow and Balthazar CT severity index scores in predicting severity of acute pancreatitis. Korean J Gastroenterol. 2011; 58: 31-7.
- Khanna AK, Meher S, Prakash S, Tiwary SK, Singh U, et al. Comparison of Ranson, Glasgow, MOSS, SIRS, BISAP, APACHE-II, CTSI Scores, IL-6, CRP, and Procalcitonin in Predicting Severity, Organ Failure, Pancreatic Necrosis, and Mortality in Acute Pancreatitis. HPB Surg. 2013; 2013: 367581.
- Dumnicka P, Sporek M, Mazur-Laskowska M, Ceranowicz P, Kuzniewski M, et al. Serum Soluble Fms-Like Tyrosine Kinase 1 (sFlt-1) Predicts the Severity of Acute Pancreatitis. Int J Mol Sci. 2016; 17: 2038.
- Gao W, Yang HX, Ma CE. The Value of BISAP Score for Predicting Mortality and Severity in Acute Pancreatitis: A Systematic Review and Meta-Analysis. PLoS One. 2015; 10: e0130412.
- Miko A, Vigh E, Matrai P, Soos A, Garami A, et al. Computed Tomography Severity Index vs. Other Indices in the Prediction of Severity and Mortality in Acute Pancreatitis: A Predictive Accuracy Meta-analysis. Front Physiol. 2019; 10: 1002.
- Chen L, Lu G, Zhou Q, Zhan Q. Evaluation of the BISAP score in predicting severity and prognoses of acute pancreatitis in Chinese patients. Int Surg. 2013; 98: 6-12.
- Bezmarevic M, Kostic Z, Jovanovic M, Mickovic S, Mirkovic D, et al. Procalcitonin and BISAP score versus C-reactive protein and APACHE II score in early assessment of severity and outcome of acute pancreatitis. Vojnosanit Pregl. 2012; 69: 425-31.