
SciBase Journals
SciBase Gastroenterology and Hepatology
- Article Type: Case Report
- Volume 1, Issue 2
- Received: Oct 16, 2024
- Accepted: Nov 19, 2024
- Published Online: Nov 26, 2024
Peutz Syndrome Involving the Cervix Masquerading as a Cervical Neoplasm: A Rare Case Report
Meng-Ling Ma; Cong-Li Liu; Jin-Ju Dong*
Department of Obstetrics and Gynecology, Xiangyang No, 1 People’s Hospital, Hubei University of Medicine, Xiangyang 441000, China.
*Corresponding Author: Jin-ju Dong
Department of Obstetrics and Gynecology, Xiangyang No, 1
People’s Hospital, Hubei University of Medicine, Xiangyang
441000, China.
Email: 296541679@qq.com
Abstract
Background: Peutz-Jeghers syndrome, also known as Peutz-Jeghers Syndrome (PJS), is a rare autosomal dominant genetic disease with an incidence of 1/200 000-1/8 300 [1]. Among them, the most common sites of tumors include gastrointestinal tract, cervix, ovary, breast, lung, pancreas, etc. The incidence of gynecological related tumors such as Gastrotype Endocervical Adenocarcinoma (G-EAC) is only 15-30%. The average age is 33 years old [2], and it is easy to be missed and misdiagnosed in clinical practice. In addition, Lobular Endocervical Glandular Hyperplasia (LEGH) is considered to be the precursor lesion of GEAC [3-10]. Therefore, we report a case of cervical involvement in a 13-year-old girl with Peutz-Jeghers syndrome, and review the clinical features, diagnosis, treatment and postoperative follow-up of the patient, in order to improve clinicians’ understanding of Peutz-Jeghers syndrome related gynecological tumors.
Case introduction: The 13-year-old girl came to the hospital due to lower abdominal pain. During the treatment of abdominal pain symptoms, CT examination revealed intussusception and incomplete intestinal obstruction, and a large cervical mass, about 3.1×2.9 cm in size was found. After the treatment of gastrointestinal surgery and obstetrics and gynecology, the postoperative disease was confirmed as Peutz-Jeghers Polyp (PJP) and the precursor lesion of cervical gastric adenocarcinoma.
Conclusion: When children with Peutz-Jeghers syndrome are complicated with cervical lesions, cervical gastric-type adenocarcinoma should be considered.
Keywords: Peutz syndrome; Gynecology; Malignant tumors; Gastric adenocarcinoma of the cervix; The endocervical glands were hyperplastic.
Citation: Ma ML, Liu CL, Dong JJ. Peutz Syndrome Involving the Cervix Masquerading as a Cervical Neoplasm: A Rare Case Report. SciBase Gastroenterol Hepatol. 2024; 1(2): 1008.
Introduction
Peutz-Jeghers Syndrome (PJS), also known as Peutz-Jeghers syndrome, is an autosomal dominant genetic disease. The main cause of PJS is the mutation of the tumor suppressor gene, serine/ threonine kinase 11 gene [3]. PJS is characterized by multiple gastrointestinal polyps and skin and mucosal pigmentation, and 50% of PJS have a family history [4]. The common sites of tumors include the gastrointestinal tract, cervix, ovary, breast gland, lung, pancreas, etc. The risk of breast and testicular tumors in PJS patients can be increased by 10 to 18 times compared with normal people [5], especially for female patients. Gynecological related tumors such as Gastric-Type Endocervical Adenocarcinoma (G-EAC) and sex cord tumor with annular tubules (FIGO) should be extra vigilant. SCTAT), whose cumulative lifetime risk was 10% and 18%-21%, respectively [6].
G-EAC belongs to a special subtype of cervical adenocarcinoma, accounting for 10%-15% [7]. Most of the lesions are highly invasive growth in the cervical canal, and the cervix is barrel shaped. There are often no macroscopic exogenous lesions in the early stage, and it is not related to Human Papilloma Virus (HPV) infection. In addition, its symptoms are less typical and lack of specificity, mainly manifested as increased vaginal discharge, rare abdominal pain and contact bleeding. Therefore, patients often ignore their own symptoms, and inex perienced clinicians may also misdiagnose it as an inflammatory disease, so that most patients are diagnosed at an advanced or advanced stage. Another characteristic of G-EAC is the susceptibility to ovarian metastasis and synchronous mucinous metaplasia and neoplasia of the female genital tract, which is also known as Synchronous Mucinous Metaplasia and Neoplasia of the Female Genital Tract (SMMN-FGT). In clinical diagnosis and treatment, attention should be paid to further pelvic imaging examination and the determination of the scope of surgery [8,9]. Importantly, G-EAC is a highly aggressive tumor with a very poor prognosis, with a 5-year disease-specific survival of only 42% compared to 92% for conventional HPV-associated cervical adenocarcinoma [10,11].
Case presentation
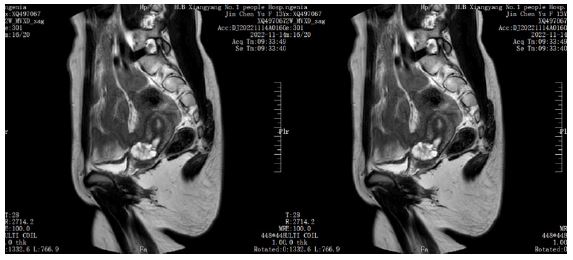
The patient was a 13-year-old female student, with no sexual history, normal health, no smoking and drinking habits, and no history of exposure to toxic and radioactive substances. Due to lower abdominal pain for 3 days, he was treated in the Department of General Surgery of Xiangyang No.1 People’s Hospital on July 7, 2022. During hospitalization, CT examination of the lower abdomen showed intussusception, incomplete intestinal obstruction, and a cervical space occupying lesion with a size of about 4.0×3.0 cm. Then the gynecological consultation was requested, and a 4.0×3.0×3.0 cm mass was palpable during anal examination. It appeared to be an enlarged cervix or mass without tenderness. Further pelvic MRI examination was recommended, and the result showed that the cervical mass was a mucinous neoplastic lesion with a size of about 3.1×2.9 cm (Figure 1). After that, the patient was fully prepared for surgical intestinal surgery. After the disease was cured, he was transferred to the Department of gynecology for further diagnosis and treatment of cervical mass on July 20, 2022. The patient had menarche at the age of 10 years and had a 7-day menstrual cycle of 50-60 days with normal menstrual volume and occasional dysmenorrhea. Normal no abdominal pain, abdominal distension, no vaginal fluid, secretion increase, peculiar smell, no frequent urination, urgency and other discomfort. Physical examination showed stable vital signs, his height was 153 cm, weight was 44 kg, and body mass index was 18.8 kg/m2. There were scattered dark spots on the mucous membrane of the mouth and lips without projecting the mucosal surface, and the rest of the skin was normal. Gynecological examination revealed a 4.0×3.0×3.0 cm mass, which seemed to be an enlarged cervix or mass, without tenderness, smooth rectal mucosa, and no blood staining on finger tips.
Previous history: The patient had been a healthy person, but had scattered dark spots on the oral mucosa in infancy, and had no discomfort symptoms. He denied the history of hepatitis, tuberculosis, hypertension, diabetes, heart disease, trauma, blood transfusion, drug and food allergy. On July 7, 2022, the patient underwent surgical treatment due to intussusception and intestinal obstruction in the General surgery Department of our hospital. The postoperative pathological examination was consistent with the histological characteristics of Peutz-Jeghers Polyp (PJP), and the patient was diagnosed with Peutz-Jeghers polyp syndrome combined with medical history characteristics. Neither the patient nor his parents underwent genetic testing.
Family history: His father was healthy. When she was about 30 years old, gastrointestinal endoscopy showed multiple gastrointestinal polyps with Peutz-Jeghers Polyp (PJP) histological characteristics. In a similar situation, my grandmother was found to have polypoid polyps and died of the disease.
Reproductive history: After completing the relevant preparations to exclude surgical contraindications, the patient underwent hysteroscopy + hysteroscopic cervical lesion resection + hysteroscopic cervical lesion resection + hysteroscopic cervical lesion unroofing on July 22, 2022. During the operation, several “hills” like cystic processes were seen in the cervical canal, and follicle-like tissue was seen in the right side of the cervical canal after the obvious tissue was cut out. All the tissues were sent for pathological examination and recovered well after operation.
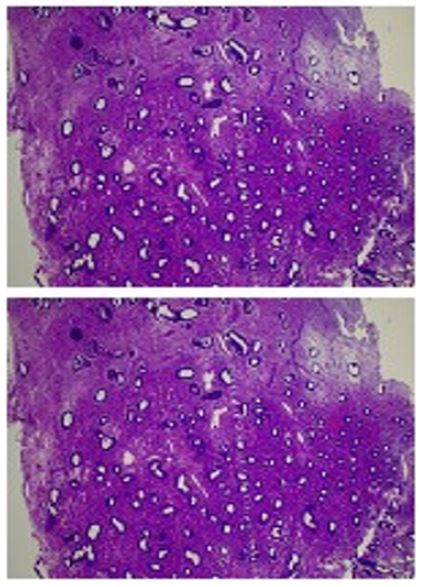
Postoperative pathological diagnosis: (lower uterine-cervical canal) hyperplasia image endometrium combined with lobular endocervical glandular hyperplasia (LEGH). IHC showed MUC5A (+), MUC-6 (+), P16 (-), CEA (-), MUC2 (-) and Ki-67 (positive rate < 5%) in hyperplastic glands. Special staining: PAS (neutral mucus +), AB-PAS (goblet cells +). Note: LEGH is a hyperplasia of endometrial glands in the cervix with small intestinal and pyloric glandular metaplasia. It has been reported that LEGH is a precursor lesion of gastric adenocarcinoma of the cervix. This case is a patient with PJ syndrome, and it is recommended to perform KRAS, STKII and other gene mutation detection and annual regular gynecological ultrasound and cervical cytology follow-up (see Figure 2).
Gene diagnosis of the family: KRAS, STKII and other gene mutations were detected after surgery, and a nonsense mutation c.454C>T (p. Gln152*, Het) was detected in the STK11 gene of the subject, which may lead to abnormal protein coding or abnormal protein coding. Taken together, this mutation was a known pathogenic mutation.
Recommendation: The detection of harmful mutations in this test will lead to an increase in the risk of related tumors. It is recommended that the subject contact a specialist or genetic counselor to develop a personalized risk management plan. In addition, the family members of the patient were recommended to verify the related loci in order to understand the risk of corresponding tumors. The family members of the patient refused to undergo genetic testing, and no family gene related loci were found. The operation process was smooth, the postoperative recovery was good, and the postoperative precautions and long-term follow-up were explained to achieve “early detection and early treatment” and reduce the occurrence of tragedy. Long-term follow-up: A series of examinations including transvaginal ultrasound and pelvic imaging examinations were performed every six months, and no disease progression was found.
Discussion
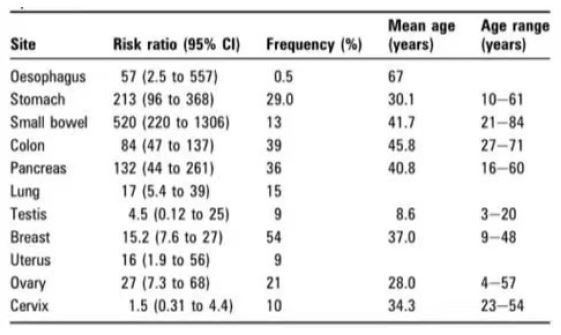
Peutz-Jeghers Syndrome (PJS) is an autosomal dominant genetic disease. The main pathogenesis is the inactivation of STK11/ LKB1 gene. STK11/LKB1 is a tumor suppressor gene located on chromosome 19p13.3 with a molecular size of about 23 KB. The gene is expressed in almost all human tissues and participates in the regulation of cellular DNA damage response, cell proliferation, senescence, apoptosis, cell differentiation and aerobic glycolysis, and inhibits tumorigenesis [2]. The loss of STK11/LKB1 will lead to the imbalance between cell survival and tumor growth inhibition, and make cells fall into the crisis of hypoxia. Some cells will therefore undergo apoptosis, while some cells will start cancer-related pathways in order to adapt to the hypoxia pressure and maintain the energy supply of cells, which will lead to abnormal cell differentiation in the long run [3]. The clinical features include multiple polyps of the gastrointestinal tract, abnormal pigmentation of the skin and mucosa of the lips, face, toes, palms and soles, and a significant increase in the risk of a variety of malignant tumors. Gastrointestinal polyps in PJS patients have a high risk of canceration, which will evolve from hamartoma to adenoma and finally malignant transformation to adenocarcinoma, thus becoming the main cause of death in PJS [4]. The risk of cancer in PJS is about 18 times higher than that in the general population, and about 85% of patients will develop malignant tumors before the age of 70 years. The most common are colorectal cancer, breast cancer, and malignant tumors in the small intestine, stomach and pancreas [5]. It is associated with lung cancer, pancreatic cancer, cervical cancer, and endometrial cancer [6] (Figure 3).
Gastric-type endocervical adenocarcinoma (GAS) was first proposed b. Japanese scholar [12] in 2007, and described as a malignant epithelial tumor of the cervix characterized by the expression of gastric-type mucus and morphologically similar to the pyloric gland epithelium. In 2014 WHO classification, it was regarded as a special type of cervical mucinous adenocarcinoma [13].
With the increasing incidence of cervical Adenocarcinoma year by year and the deepening of understanding of it, the International Endocervical Adenocarcinoma Criteria and Classification, 2018, IECC) proposed that cervical adenocarcinoma should be divided into Human Papillomavirus (HPV)-related type and non-HPV related type according to clinical biological behavior and etiology, while GAS is the most common subtype of non-HPV related type [14]. The clinical manifestations are extremely atypical, and screening is difficult, which is easy to be missed and misdiagnosed, delaying the diagnosis and treatment, and the prognosis is poor. In the past 10 years, with the continuous research on GAS, more and more scholars believe that cervical gastral adenopathy is a spectrum of lesions including benign lesions, precancerous lesions and cancer [15]. The precursor lesions of GAS include Lobular Endocervical Glandular Hyperplasia (LEGH), atypical LEGH, cervical gastric Adenocarcinoma In Situ (gAIS) and Peutz-Jeghers Syndrome (PJS), and attention should be paid to its management. Identification and management of precursor lesions are essential for cancer prevention and early detection. PJS patients received gynecological ultrasound examination, gynecological examination and cervical cytology every year from the age of 18 to 20 years (those with sexual history). The name Lobular Endocervical Glandular Hyperplasia (LEGH) was first proposed by [16] in 1999. It was described as a cervical pseudotumor-like lesion similar to Minimal Deviation Adenocarcinoma (MDA). Almost at the same time, [17] also reported 3 cases of similar lesions, which were described as endometrial gland hyperplasia with small intestine and pyloric gland metaplasia, and found that these glands had neutral mucus positive for Periodic Acid-Schiff (PAS) staining and gastric pyloric gland immunophenotype positive for anti-αGlcNAc (clone number HIK1083). It was not until 2003 that the two teams reached a consensus to use LEGH to replace the description of pyloric glandular metaplasia [18]. LEGH is not a common lesion; A single-center study reported that the incidence of LEGH was only 0.7% among 1169 Japanese female patients undergoing total hysterectomy, and LEGH was considered to be a metaplastic change [19]. Another 2 groups reported that 13 and 3 patients with LEGH lesions were followed up for an average of 3.4 and 4 years, respectively, and no recurrence was found, thus the lesions were considered to be benign [16,17]. However, it has been reported that LEGH is a precursor lesion of GAS, rather than a metaplastic change. Because LEGH can be observed simultaneously in many cases of G-EAC [20]. Some subsequent molecular studies also found that LEGH and its coexisting G-EAC/MDA had some of the same genetic changes, such as GNAS, STK11 and KRAS mutations, which suggested that LEGH might transform or progress to GAS [21]. Some studies have also shown that LEGH often coexists with MDA, and both of them are positive for HIK1083 immunohistochemistry, suggesting that LEGH may be a precancerous lesion of MDA. In addition, molecular pathological studies have also found that some LEGH have a base deletion in exon 6 of STK11/LKB1, which further supports that LEGH may be a precancerous lesion of MDA and may be one of the phenotypes of PJS [10]. However, there is no definite conclusion on this point of view. In summary, LEGH is a rare form of glandular hyperplasia in the cervical canal, and is officially classified as benign glandular tumors and tumor-like lesions of the cervix by WHO [11].
Atypical LEGH, gastric adenocarcinoma in situ of cervix: [22] first reported atypical LEGH, and they also found atypical LEGH lesions in 6 out of 20 cases of MDA. Another study using comparative genomic hybridization revealed the same chromosomal instability (including 3q amplification and 1p loss) as in MDA in 3/14 LEGH, it is supported that at least part of LEGH is a precancerous or prodromal lesion of GAS [23]. In 2013, Mikami and McCluggage [23] referred to cervical adenocarcinoma in situ with nuclear atypia and gastric type phenotypes as gAIS. In 2017, [24] reported 9 cases of gAIS with the largest sample size and summarized their morphological characteristics. At present, although gAIS has been recognized as a prodromal lesion of cervical GAS, it has a high rate of missed diagnosis due to its low incidence. It should be noted that atypical LEGH or gAIS may appear independently and not all accompany GAS [14]. Found [24] that a patient who underwent cervical polypectomy progressed to GAS 6 years later, and the polyp specimen was retrospectively diagnosed as gAIS. Gastro-type endocervical adenocarcinoma (GAS): The incidence and global distribution of GAS are unknown. Reports on the proportion of GAS in cervical adenocarcinoma are different, such as 10% in international studies [14], 25%-28% in Japan [16], and 1.5% in Europe [18]. It is generally believed that GAS is the second most common cervical adenocarcinoma after usual HPV associated endocervical adenocarcinoma (UEA). The age of GAS patients ranged from 37 to 84 years (mean 49 years). The main clinical manifestations were abnormal vaginal discharge and bleeding. Clinical examination shows cervical hypertrophy, the so-called “barrel” cervix, but some cases may have a normal appearance at colposcopy [15]. Compared with UEA, GAS is more aggressive and usually manifests as deep tumor stromal invasion, lymphovascular invasion, lymph node metastasis, ovarian involvement, other pelvic organ involvement, and peritoneal dissemination [25,26]. However, there was no significant difference in the above indicators between MDA and non-MDA GAS [26], indicating that the degree of differentiation of GAS has nothing to do with the degree of malignancy [25]. GAS is mostly in the advanced stage (stage ⅱ-ⅳ) [25,26] and has a poor prognosis. The newly reported cases of GAS were collected from 2007 to 2007, and the average follow-up time was 30-42 months. Analyzing the prognosis of GAS patients, we found that GAS was more likely to relapse and distant metastasis than UEA [25]. The 5-year Disease-Free Survival (DFS) and 5-year Disease-Specific Survival (DSS) of GAS were significantly lower than those of UEA (DFS: 25% vs. 75% [16]; DSS: 30% vs. 77% [16], 42% vs. 91% [26]). Peutz-jeghers syndrome (PJS) is an autosomal dominant genetic disease, which is associated with mucocutaneous pigmentation and gastrointestinal dysplastic polyps. Lesions of PJ syndrome in the female reproductive system include GAS, ovarian mucinous tumors, and Sex Cord Tumors with Annular Tubule (SCTAT) [27]. STK11/LKB1 is not only considered a tumor suppressor gene associated with the development of PJ syndrome, but its genetic abnormalities are also present in the spectrum of cervical gastrotype lesions ranging from benign to malignant as described previously. The incidence of GAS in patients with PJ syndrome is estimated to be 15%-30%, and the average age of onset is 33 years. Therefore, it is recommended that patients with PJ syndrome undergo regular gynecological ultrasound and cervical cytology examination every year. About 14% of GAS patients are accompanied by PJ syndrome. Pathologists should inform clinicians and patients of the possible risk of PJ syndrome when diagnosing GAS, and genetic counseling and detection of related molecular biological indicators are recommended [27]. Patients with LEGH or MDA/GAS sometimes develop multifocal mucinous lesions in 2 or more sites in the female reproductive tract. It is called Synchronous Mucinous Metaplasia and Neoplasia of the Female Genital Tract (SMMN-FGT) [28]. These lesions may be mucinous metaplasia of the endometrium, fallopian tubes, or ovaries, or they may be mucinous neoplasms. Some cases are accompanied by appendiceal mucinous cystadenoma and bladder mucinous metaplasia, and some patients have PJ syndrome at the same time [29]. At present, there is no treatment principle for GAS based on histopathological types and molecular pathological characteristics. The 2018 National Comprehensive Cancer Network (NCCN) Clinical practice guideline for cervical cancer recommends that the treatment for patients with cervical adenocarcinoma is similar to that for patients with squamous cell carcinoma of the same stage, that is, for stage ⅠB1 and ⅡA1 patients can only undergo radical hysterectomy. For patients with stage ⅠB2, ⅡA2 and ⅱb-ⅳA, platinum-based concurrent chemoradiotherapy on the basis of radical surgery is recommended [30]. Although the 2020 NCCN guidelines update the treatment principles of ordinary cervical adenocarcinoma according to its histopathological classification, it only recommends that such patients should not undergo fertility-preserving surgery [31]. The clinical treatment study of [26] found that GAS patients had resistance to docetaxel and carboplatin regimens. Moreover, compared with UEA patients, GAS patients had more obvious chemoresistance (85.0% vs. 46.2%) [30]. Therefore, scholars generally believe that the poor prognosis of GAS may be related to its difficult detection and chemotherapy resistance. To improve the prognosis of GAS patients, the existing treatment strategy should be changed and the specific chemotherapy strategy of GAS, namely molecular targeted therapy strategy, should be established [30]. In view of the early age of onset and high risk of cancer in PJS patients, the American College of Gastroenterology (ACG) recommends that PJS patients should be regularly monitored from a young age [32]. Among them, the gastrointestinal tract should be examined by colonoscopy every 3 years, and the female reproductive system should be examined more closely, such as the ovary, uterus, cervix and so on. A series of related examinations including transvaginal ultrasound, pelvic imaging examination and cervical cytology should be performed annually from the age of 18 to 20 years. It is recommended that patients’ family members should be screened for various tumors at different ages to achieve the purpose of early diagnosis and early treatment. In conclusion, PJS is a rare clinical syndrome, and PJS-related diseases of the female reproductive system are even rarer. At present, the mechanism of these diseases is not fully understood, so the accumulation of more cases and even multi-center joint research are needed. By reviewing the clinical characteristics, diagnosis and treatment process and postoperative follow-up of this patient, we hope to improve clinicians’ understanding of Peutz-Jeghers syndrome and its related gynecological tumors, so as to reduce the missed diagnosis of the disease, find the disease as soon as possible, and achieve the purpose of early diagnosis and treatment.
References
- Tacheci L, Kopacova M, Bures J, et al. Peutz-Jeghers syndrome J. Curr Opin Gastroenterol, 2021, 37(3): 245-254. Doi:10.1097/MOG. 0000000000000718.
- Banno K, Kisu I, Yanokura M, et al. Hereditary gynecological tumors associated with Peutz-Jeghers syndrome (Review) J. Oncol Lett. 2013; 6(5): 1184-1188.
- Shah J, Sunkara T, Xiao P, et al. Peutz-Jeghers Syndrome Presenting as Colonic Intussusception: A Rare Entity J. Gastroenterology Res. 2018; 11(2): 150-153.
- Akseli Hemminki, David Markie, Ian Tomlinson, et al. A serine/threonine kinase gene defective in Peutz-Jeghers syndrome J. Nature. 1998; 6663(391): 184-187.
- Hearle N, Schumacher V, Menko FH, et al. Frequency and spectrum of cancers in the Peutz-Jeghers syndrome J. Clin Cancer Res. 2006; 12(10): 3209-3215.
- Gupta S, Provenzale D, Llor X, et al. NCCN guidelines insights, genetic/familial high-risk assessment: Colorectal, version 2. 2019 J. J Natl Compr Canc Netw. 2019; 17(9): 1032-1041.
- Xu H, Zhang J. Interpretation of the pathological content update of the 2020 clinical practice guideline for cervical cancer from the National Comprehensive Cancer Network J. Chin J Pathology. 2021; 50(1): 9-13.
- Wang Dengfeng, Zhang Guonan, Shi Yu et al. Clinical analysis of 11 cases of gastric adenocarcinoma of the cervix J. Cancer Prevention and Treatment. 2021; 34(5): 431-437.
- Zhang GN, Wang DF. Pay attention to the diagnosis and treatment of cervical gastric adenocarcinoma and improve the level of precision diagnosis and treatment J. Chin J Practical Gynecology & Obstetrics. 2021; 37(1): 25-28.
- Karamurzin YS, Kiyokawa T, Parkash V, et al. Gastric-type endocervical adenocarcinoma J. Am J Surg Pathol. 2015; 39: 1449-1457.
- McCluggage WG, Harley I, Houghton JP, et al. Composite cervical adenocarcinoma composed of adenoma maligned and gastric type adenocarcinoma (dedifferentiated adenoma malig‐ num) in a patient with Peutz-Jeghers syndrome J. J Clin Pathol. 2010; 63: 935-941.
- Kojima A, Mikami Y, Sudo T, et al. Gastric morphology and immunophenotype predict poor outcome in mucinous adenocarcinoma of the uterine cervix J. Am J Surg Pathol. 2007; 31(5): 664-672.
- Kurman RF, Carcangiu ML, Herrington CS, et al. WHO classicification of tumours of female reproductive organs M. Lyon: IARC Press. 2014: 183-194.
- Stolnicu S, Barsan I, Hoang L, et al. International Endocervical Adenocarcinoma Criteria and Classifiction (IECC): A new pathogenetic classification for invasive adenocarcinomas of the endocervix J. Am J Surg Pathol. 2018; 42(2): 214-226.
- Talia KL, McCluggage WG. The developing spectrum of gastric-type cervical glandular lesions J. Pathology. 2018; 50(2): 122-133.
- Nucci MR, Clement PB, Young RH. Lobular endocervical glandular hyperplasia, not otherwise specified: A clinicopathologic analysis of thirteen cases of a distinctive pseudoneoplastic lesion and comparison with fourteen cases of adenoma malignum J. Am J Surg Pathol. 1999; 23(8): 886-891.
- Mikami Y, Hata S, Fujiwara K, et al. Florid endocervical glandular hyperplasia with intestinal and pyloric gland metaplasia: Worrisome benign mimic of adenoma malignum J. Gynecol Oncol. 1999; 74(3): 504-511.
- Mikami Y. Gastric-type mucinous carcinoma of the cervix and its precursors-historical overview J. Histopathology. 2020; 76(1): 102-111.
- Mikami Y, Hata S, Melamed J, et al. Lobular endocervical glandular hyperplasia is a metaplastic process with a pyloric gland phenotype J. Histopathology. 2001; 39(4): 364-372.
- Ohta Y, Suzuki T, Hamatani S, et al. Lobular endocervical glandular hyperplasia might become a precursor of adenocarcinoma with pyloric gland features J. Pathol Res Pract. 2008; 204(9): 683-687.
- Ando H, Miyamoto T, Kashima H, et al. Usefulness of a management protocol for patients with cervical multicystic lesions: A retrospective analysis of 94 cases and the significance of GNAS mutation J. J Obstet Gynaecol Res. 2016; 42(11): 1588-1598.
- Mikami Y, Kiyokawa T, Hata S, et al. Gastrointestinal immunophenotype in adenocarcinomas of the uterine cervix and related glandular lesions: A possible link between lobular endocervical glandular hyperplasia/pyloric gland metaplasia and ′adenoma malignum′ J. Mod Pathol. 2004; 17(8): 962-972.
- Kawauchi S, Kusuda T, Liu XP, et al. Is lobular endocervical glandular hyperplasia a cancerous precursor of minimal deviation adenocarcinoma? A comparative molecular-genetic and immunohistochemical study J. Am J Surg Pathol. 2008; 32(12): 1807-1815.
- Talia KL, Stewart C, Howitt BE, et al. HPV-negative gastric type adenocarcinoma in situ of the cervix: A spectrum of rare lesions exhibiting gastric and intestinal differentiation J. Am J Surg Pathol. 2017; 41(8): 1023-1033.
- Nishio S, Mikami Y, Tokunaga H, et al. Analysis of gastric-type mucinous carcinoma of the uterine cervix -an aggressive tumor with a poor prognosis: a multi-institutional study J. Gynecol Oncol. 2019; 153(1): 13-19.
- Karamurzin YS, Kiyokawa T, Parkash V, et al. Gastric-type endocervical adenocarcinoma: An aggressive tumor with unusual metastatic patterns and poor prognosis J. Am J Surg Pathol. 2015; 39(11): 1449-1457.
- Meserve EE, Nucci MR. Peutz-Jeghers syndrome: Pathobiology, pathologic manifestations, and suggestions for recommending genetic testing in pathology reports J. Surg Pathol Clin. 2016; 9(2): 243-268.
- Mikami Y, McCluggage WG. Endocervical glandular lesions exhibiting gastric differentiation: an emerging spectrum of benign, premalignant, and malignant lesions J. Adv Anat Pathol. 2013; 20(4): 227-237.
- Ikeda Y, Yasuda M, Kato T, et al. Synchronous mucinous metaplasia and neoplasia of the female genital tract with external urethral meatus neoplasm: A case report J. Gynecol Oncol Rep. 2015; 12: 27-30.
- Kojima A, Shimada M, Mikami Y, et al. Chemoresistance of gastric-type mucinous carcinoma of the uterine cervix: A study of the sankai gynecology study group J. Int J Gynecol Cancer. 2018; 28(1): 99-106.
- Nakamura A, Yamaguchi K, Minamiguchi S, et al. Mucinous adenocarcinoma, gastric type of the uterine cervix: Clinical features and HER2 amplification J. Med Mol Morphol. 2019; 52(1): 52-59.
- Syngal S, Brand RE, Church JM, et al. ACG clinical guideline: Genetic testing and management of hereditary gastrointestinal cancer syndromes. Am J Gastroenterol. 2015; 110(2): 223-262.