
SciBase Journals
SciBase Gastroenterology and Hepatology
ISSN 2691-7785
- Article Type: Short Report
- Volume 2, Issue 1
- Received: Jan 21, 2025
- Accepted: Feb 28, 2025
- Published Online: Mar 07, 2025
Metachronous aggressive large B-cell non hodgkin lymphoma of the stomach in a patient wıth prostate carcinoma
Hamarat H*; Özgeyik MO
Department of Internal Medicine, Eskişehir City Hospital, Turkey.
*Corresponding Author: Hamarat H
Departmen of Internal Medicine, Eskişehir City Hospital, Eskişehir, Turkey.
Email: hklncal@hotmail.com
Citation: Hamarat H, Ozgeyik MO. Metachronous aggressive large B-Cell non hodgkın lymphoma of the stomach in a patient with prostate carcinoma. SciBase Gastroenterol Hepatol. 2025; 2(1): 1009.
Short report
In this correspondence, we present a case of aggressive large B-cell Non-Hodgkin’s Lymphoma (NHL) diagnosed in the stomach of a patient undergoing hormone therapy for prostate carcinoma.
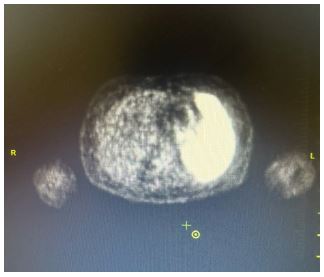
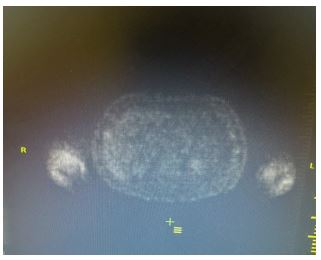
A 57-year-old male patient presented to the internal medicine outpatient clinic with complaints of weight loss, anorexia and early satiety that had lasted for a period of two months. The patient had been diagnosed with prostate carcinoma and was undergoing Gonadotropin-Releasing Hormone (GnRH) agonist treatment. On physical examination, the patient was conscious, orientated. The patient appeared pale and weak. The patient’s vital signs revealed a blood pressure of 90/60 mmHg, a pulse rate of 114 beats per minute, and an oxygen saturation level of 98%. Abdominal examination revealed tenderness in the gastric region, while additional examination findings were unremarkable. Laboratory analysis revealed the following results: haemoglobin 6.8 g/dL, haemotocrit 25.6%, MCH 15.8 pg and MCV 69.6 fL. Biochemical parameters were found to be within normal limits. Serum ferritin levels were found to be 10 μg/L, while vitamin B12 levels were recorded at 216 ng/L. Furthermore, coagulation tests, acute phase reactants, hepatitis and HIV markers were found to be negative. Direct Coombs, LDH, and Haptoglobin levels were found to be within normal parameters. A peripheral smear revealed no signs of pathological cells, but did indicate iron deficiency anaemia. The patient was evaluated for gastrointestinal bleeding, but no such bleeding was detected. The patient was admitted to the internal medicine ward on the basis of anaemia and oral intake disorder, and treatment was initiated. Abdominal ultrasonography revealed no abnormalities. An upper gastric endoscopy was performed to investigate the aetiology of the anaemia, revealing an ulcerated area in the large curvature region of the gastric corpus. Consequently, a biopsy was taken from this area, and the following stains were found to be diffusely positive: CD45(LCA) (Clone Roche RP2-18), MUM-1, PAX-5, CD20 (Clone Roche L26), CD79a, Bcl-6. In addition, 40% staining with C-myc was observed. Conversely, staining for CyclinD1 (Clone Roche SP4-R), Pankeratin, CD30, CD23 (Clone Roche SP23), ALK, CD10 (Clone Roche SP67) was negative. Non-neoplastic T lymphocytes were stained with CD3 (Clone Roche 2GV6) and CD5. The proliferation index with Ki-67 is 95%. Conversely, EBER staining, utilised in conjunction with the chromogenic in situ hybridisation method, yielded a negative result. Furthermore, both the TdT stain and the Helicobacter pylori stain returned negative results. The histopathological findings observed in the sections prepared from the gastric corpus marked material, in conjunction with the results of immunohistochemical staining, allowed for the diagnosis of aggressive large B-cell non-Hodgkin’s lymphoma. Positron Emission Tomography-Computed Tomography (PET-CT) was performed for lymphoma staging, revealing involvement in all lymph nodes and the spleen, consistent with lymphoma (Figure 1). R-CHOP regimen chemotherapy was initiated as a treatment.No involvement was detected in the control PET-CT of the patient whose chemotherapy treatment had concluded (Figure 2).
Consequently, a marked increase in the number of cancer survivors has been observed [1]. In 2-17% of cancer survivors, another primary cancer was detected in time [2]. All types of non-Hodgkin’s lymphoma can be detected synchronously or metachronously as primary cancer. Examples of this are documented in the literature [3-5]. There are also cases of nongastric non-Hodgkin’s lymphoma detected metachronously with localised prostate carcinoma [6]. The present patient had gastric lymphoma. A thorough review of the literature failed to reveal any analogous cases.
Gastric large B-cell lymphoma is a rare form of lymphoma, the clinical presentation of which is often non-specific [7]. It is most commonly associated with Helicobacter Pylori (HP) infection, although there may be occasional cases in which HP infection is not present, as evidenced by the present case. In patients with another primary cancer, detailed investigations should not be avoided in the presence of nonspecific findings. In the case presented, the patient had a diagnosis of prostate cancer and was undergoing hormone therapy, thus the presence of anemia and dyspeptic complaints does not constitute alarm symptoms. Nevertheless, the presence of a secondary cancer constitutes an indication for a detailed imaging examination for the patient. In this particular case, the primary indication for the upper GI endoscopy was the presence of dyspeptic symptoms and anaemia. The endoscopy findings revealed a malignant appearance, and the pathology was consistent with gastric large B-cell lymphoma. A PET-CT scan was performed to determine the staging and to inform treatment planning, revealing the presence of multiple lymph node and splenic involvement. Following the administration of treatment, the patient entered a state of remission.
The present case study demonstrates an association of particular interest: Specifically, a male patient was diagnosed with gastric large B-cell lymphoma, accompanied by systemic involvement that was not associated with Helicobacter pylori infection. The diagnosis was made possible by the use of imaging techniques, which played a critical role in the identification of non-specific clinical findings. It is imperative to emphasise non-specific findings in patients with primary cancer.
References
- Global Cancer Observatory. 2023. Available online: https://gco.iarc.fr/en.
- Vogt A, Schmid S, Heinimann K, Frick H, Herrmann C, Cerny T, et al. Multiple primary tumours: Challenges and approaches, a review. ESMO Open. 2017; 2: e000172.
- Hanna F, Prakash A, Allan E, Khalafallah AA. Successful treatment of concomitant metastatic prostate cancer and B-cell non-Hodgkin’s lymphoma with R-EPOCH chemotherapy regimen and antiandrogen therapy. BMJ Case Rep. 2018; 2018: bcr2017223637.
- Popivanov GI, Bochev P, Hristoskova R, Mutafchiyski VM, Tabakov M, Philipov A, et al. Synchronous papillary thyroid cancer and non-Hodgkin lymphoma: Case report. Medicine (Baltimore). 2018; 97: e9831.
- Yao KL, Yu ZQ, Jin K, Wu JJ, Wang L. Synchronous primary gastric diffuse large B-cell lymphoma and multiple lung primary adenocarcinoma with pulmonary cryptococosis: a case report and literature review. BMC Pulm Med. 2024; 24: 528.
- Kalender ME, Sevinc A, Tutar E, Buyukberber S, Camci C. Metachronous non-Hodgkin’s lymphoma in a patient with localized prostate cancer. Med Oncol. 2007; 24: 466–468.
- Juarez-Salcedo LM, Sokol L, Chavez JC, Dalia S. Primary gastric lymphoma: epidemiology, clinical diagnosis, and treatment. Cancer Control. 2018; 25.