
SciBase Journals
SciBase Hematology & Blood Disorders
- Article Type: Research Article
- Volume 1, Issue 1
- Received: July 20, 2024
- Accepted: Sep 18, 2024
- Published Online: Sep 25, 2024
Investigation of Entamoeba Histolytica among Food-Handler in Erbil City - Iraq
Ahmed Akil Al-Daoody*; Fattma A Ali*; Gashbin Ali Khalid; Avan Sharif Awlla; Rayan Esmail Aziz; Zhyan Hassan Asaad
1College of Health Sciences, Hawler Medical University, Erbil, Iraq.
2Laboratory Department, AMR Unit, Maternity Teaching Hospital, Erbil, Iraq.
3Microbiology, Education College, Salahaddin university, Iraq.
*Corresponding Author: Al-Daoody AA & Fattma A Ali
College of Health Sciences, Hawler Medical University, Erbil, Iraq.
Email: ahmed.akil@hmu.edu.krd & fattma.ali@hmu.edu.krd
Abstract
Background: The intestinal parasite of Entamoeba histolytica are among the major causes of amoebiasis throughout the world. Despite the remarkable development of diagnostic methods for parasitic diseases and the continuous awareness of their treatment and control, which led to a clear reduction in the spread of these diseases in a number of developed and industrial countries. However, parasitic diseases of all types continue to be a major health problem in many countries.
Methods and objective: Detection of Entamoeba histolytica was done by macroscopically and microscopically. The stool samples should be evaluated macroscopically by naked eyes in terms of color, forms of stool, odor, white blood cells (pus), blood and presence of mucus in stool samples. Microscopic examination was done by using direct smear with either normal saline or iodine wet mount. This study was performed to investigate the prevalence and risk of Entamoeba histolytica among food handlers in Erbil city.
Results: Out of (23600) samples examined, 845 (3.6%) were positive by using direct wet mount examination, the parasitic species found in the fecal sample were Entamoeba histolytica (3.6%), Giardia lamblia (1.1%). The prevalence rate of parasitic infection among males (3.8%) was higher than females (2.5%) with a statistically significant difference. According to months the result showed no significant difference, but the highest rate of infection was recorded in march (5%) and lowest rate was observed in July (1.9%). According to age group the result showed no significant difference, but the highest distribution was observed in the age (16-25) (5.5%) followed by age (46-55) (3.3%), while the lowest distribution was observed in the age (36- 45) (2.6%).
Conclusion: According to our study throughout the year, Entamoeba histolytica has the highest rate followed by Giardia lamblia with male being more commonly infected.
Keywords: Stool examination; Entamoeba histolytica; Giardia lamblia; Erbil; Iraq.
Citation: Al-Daoody AA, Ali FA, Khalid GA, Awlla AS, Aziz RE, et al. Investigation of Entamoeba histolytica among Food-Handler in Erbil City - Iraq. SciBase Hematol Blood Disord. 2024; 1(1): 1004.
Introduction
Entamoeba histolytica is a protozoan parasite that causes intestinal amebiasis or amoebic dysentery as well as extra intestinal manifestations. Although 90% of E. histolytica infections are asymptomatic, nearly 50 million people become symptomatic, with about 100,000 deaths yearly [1,2].
Amoebiasis may present with no symptoms or mild to severe symptoms, including abdominal pain, diarrhea, or bloody diarrhea. Severe complications may include inflammation and perforation, resulting in peritonitis. People affected may develop anemia. If the parasite reaches the bloodstream, it can spread through the body and end up in the liver, causing amoebic liver abscesses [3].
Entamoeba histolytica is an invasive enteric protozoan. Infection typically begins with the ingestion of mature, quadrinucleated cysts found in fecally contaminated food or water [4]. Excystation occurs in the small intestine with the release of motile trophozoites, which migrate to the large intestine. Through simple binary fission increase in number and become colonized in large intestine, and both stages are shed in feces, but only cysts have the potential to transmit disease due to the protection conferred by their wall. Cysts can survive days to weeks in the external environment, while trophozoites are rapidly destroyed once outside the body or by gastric secretions if ingested [5,6].
Trophozoites have the capacity to adhere and lyse the colonic epithelium and subsequently spread hematologically through the portal vein system to distant sites such as the peritoneum, liver, lung, or brain [7]. Entamoeba histolytica infection is begun by parasite adherence to the colonic mucus membrane layer. Trophozoites express a galactose and N-acetyl-d-galactosamine specific protein (Gal/GalNAc lectin) on the cell surface and attach to host mucus membrane layer and colonic epithelial cells [8]. The colonized parasites are capable of extreme tissue destruction. In addition to the pore-forming proteins, amoebapores. hydrolytic enzymes, particularly Cysteine Proteases (CP), are considered to be essential weapons of the parasite to penetrate the epithelium and destroy components of the host’s extracellular matrix [9]. Amebic trophozoites interact directly and indirectly with host immune and non-immune cells, during and after penetration into the submucosal region [10].
Dysentery is the most common associated symptom, present in nearly 40% of affected patients [11]. Leukocytosis, and elevated alkaline phosphatase on laboratory evaluation are usually present and imaging reveals an abscess, typically on the right hepatic lobe [12].
Amebic liver abscess (ALA) is the most common extra intestinal manifestation of amoebiasis. Approximately 50-80% of individuals with ALA will present with symptoms within 2 to 4 weeks, with fever and constant, aching right upper quadrant pain. In up to 50% of cases, patients present more chronically with protracted diarrhea, weight loss, and abdominal pain [7]. The lungs are the second most common extra intestinal organ affected. Pulmonary amoebiasis generally occurs by direct extension of an ALA but can also occur by direct hematogenous spread from intestinal lesions or by lymphatic spread. The right lower or middle lobe of the lung is most commonly affected. Pulmonary abscesses, Broncho hepatic fistula, can occur when a liver abscess ruptures into the pleural space. Patients characteristically present with “anchovy sauce-like” like pus or sputum. The presence of bile in these secretions indicates liver origin [13].
Rupture of the liver abscess into the pericardium is also a rare complication with high mortality. Symptoms include severe chest pain, shortness of breath, and edema from congestive heart failure or constrictive pericarditis [14].
Risk factors that are associated with increased disease severity and mortality include young age, pregnancy, malignancy, malnutrition, alcoholism, and corticosteroid use [1]. Cause the lack of information about the spread of this parasite, and to fill the void we have done this study. To investigate the overall amoebiasis infection among food handlers in Erbil City, Distribution of amoebiasis infection according to gender and months and to detect single and double infection.
Materials and methods
The study was carried out from January 2022 to December 2022 in Erbil City at Central laboratory. A total sample were taken from (23600) individuals (19262 males, 4338 females), from different age groups were randomly chosen to be included in this study.
A fresh stool sample was collected in a clean sterile screwtop plastic container [15]. Specimens must reach the laboratory very soon (i.e., within half an hour) after passage, if this is not possible, the specimen must be treated with preservatives, the specimen container should be clearly labeled with the patient’s name, date, and time of passage of the specimen [16,17].
The stool sample should not be contaminated with urine or water, because trophozoite will be destroyed, often, multiple samples are collected and tested, these should be collected at different times on different days because parasites are shed intermittently and may not be in the stool or other samples at all times [15].
The stool samples should be evaluated macroscopically in terms of color (e.g. Brown. Yellow, or other abnormal color), the normal color is brown due to the presence of bilirubin and bile, in infants the stool may be green, its consistency may be watery or pasty [18]. Forms of stool (liquid stool, semi-formed stool and formed stool), odor (foul smelling stool may be a sign of infection), white blood cells (pus), blood and presence of mucus in stool samples, the presence of a small amount of mucus in stool is normal, however, the presence of copious mucus or bloody mucus is abnormal [19].
Microscopic examination should be performed in stool samples obtained from the area with mucus, for moving organisms, fresh stool can be examined immediately, if it is not possible to examine it should be kept in 10% formalin, the smallest amount of stool required to intensified and stained with iodine in order to detect cysts, in invasive intestinal amoebiasis, blood is generally present in stool samples [20]. Microscopic examination is done by using direct smear with either normal saline or iodine wet mount [21].
The data collected throughout the year has been coded using special designed system and entered into Microsoft excel sheets. Results were expressed as numbers and percentages. imported to statistical software Statistical Package for the Social Sciences (SPSS) version 23. The association between two variables in this study was analyzed and assessed by chi-square test. T-test used to investigate the difference between two groups, P-value< 0.05 were considered as statically significant, while result >0.05 were considered as statically insignificant.
Results
Total number of amoebic infection by using direct smear in Erbil City
The overall percentage of infection was 845 (3.6%) from (23600) samples were examined in current study in the Central laboratory in Erbil city for Entamoeba histolytica by using direct smear, as shown in Figure 1.
Prevalence of amoebic infection in relation to gender
The higher percentage of amoebic infection was observed among males (3.8%) than females (2.5%), and the difference was statistically significant (P-value=0.0384) using Chi-square as seen in Table 1.
Table 1: Prevalence of amoebic infection according to gender among Erbil City.
| Gender | No. of sample | Positive Samples | Negative Samples | P-value> | ||
|---|---|---|---|---|---|---|
| No. +ve | (%) | No. -ve | (%) | |||
| Male | 19262 | 735 | 3.8 | 18527 | 96.2 | 0.0384 |
| Female | 4338 | 110 | 2.5 | 4228 | 97.5 | |
| Total | 23600 | 845 | 3.6 | 22755 | 96.4 | |
Distribution of amoebic infection according to the months of the study
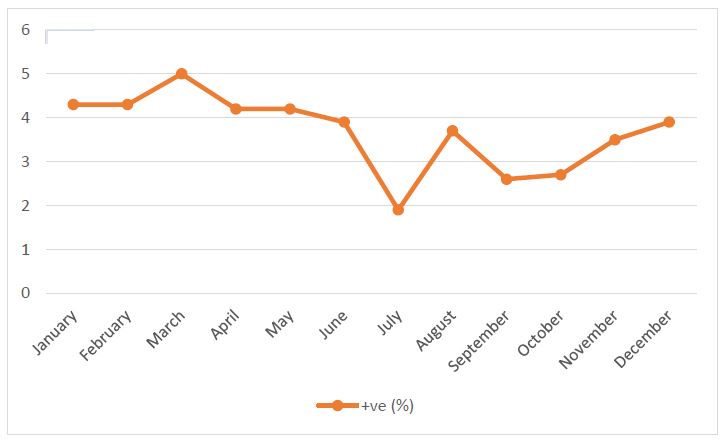
As shown in (Figure 2), the highest distribution was observed in March (5%) followed by January and February (4.3%) for each, while the lowest distribution was observed in July (1.9%), the differences statistically was non-significant (P-value = 5.189) using T-test.
Distribution of amoebic infection according to the age
As shown in (Table 2), the highest distribution was observed in the age (16-25) (5.5%) followed by age (46-55) (3.3%), while the lowest distribution was observed in the age (36-45) (2.6%), the differences statistically was non-significant (P-value=2.945) using T-test.
Table 2: Prevalence of amoebic infection according to the age.
| Age | P-value | |||||
|---|---|---|---|---|---|---|
| Age | No. +ve | +ve % | No. -ve | -ve % | Total | |
| (16-25) | 283 | 5.5 | 4851 | 94.5 | 5134 | 2.945 |
| (26-35) | 199 | 3.2 | 5955 | 96.8 | 6154 | |
| (36-45) | 141 | 2.6 | 5351 | 97.4 | 5492 | |
| (46-55) | 222 | 3.3 | 6598 | 96.7 | 6820 | |
| Total | 845 | 3.6 | 22755 | 96.4 | 23600 | |
Total number of amoebiasis and giradiasis infection by using direct smear in Erbil City
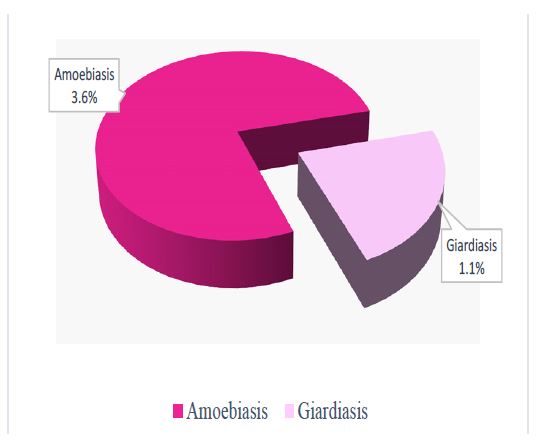
After examined a total of (23600) samples in the Central laboratory in Erbil City for Entamoeba histolytica, also we detect Giardia lamblia in this research using direct smear. The overall percentage of infection was 845 (3.6%) amoebic infection and 247 (1.1%) giardiasis infection from (23600) investigated as shown in Figure 3.
Discussion
One of the important health problem in human are parasitic infection, the prevalence rates are different according to life level, behavior style and hygienic level [22,23]. Entamoeba histolytica remains an important pathogen in many populations of the world [24].
In our study about Entamoeba histolytica among food handlers we collected a total of (23600) samples among Central laboratory in Erbil City were (19262) males and (4338) females included for prevalence of parasitic infection during one year, from January to December 2022, (845) samples were positive (3.6) (Figure 1).
Similar result was observed by previous studies, which were done in United Arab Emirates (3.3%) by [25] and (4.2%) [26]. Whereas higher result was recorded in both Duhok and Erbil cities (26.1% and 22.8%) by [22] and in India (70.7%) by [27].
The differences in these results may be due to environmental, nutritional, socio-economic, geographical condition, and health related behavior as well as lack of laboratories technician’s education on parasitic infection, or lack of technicians which has efficiency to diagnosis parasites, or that different studies may be using different methods to diagnosis parasites or there are differences of the experience of laboratory experience [28].
According to gender, the percentage of Amoebiasis infection in males (3.8%) was higher than in females (2.5%) and this difference was statistically significant (P-value=0.0384) (Table 1). Similar result was obtained by other study carried out in Mosul City by [29].
Opposite result was obtained by other studies carried out in Negeria by [30] and Saudi Arabia by [31] in which the ratio of positive females was higher than males. While another study like that of Baghdad province/Iraq by [32] have shown no significant difference between males and female’s positive rates of parasitic infection.
It is well known that the intestinal parasitic infections are in close relation to the poor sanitary habits and lack access to safe potable water and improper hygiene, the high prevalence rate of intestinal protozoa infection observed among males can be attributed to the fact that males are more active, mobile and integrated into the environment [33].
According to months our study in comparison to the study of [34], was somehow similar as both are non-significant. While was different from the study in Kuwait by [35].
Although the different months were differ in results, these may be due to people do specific activities in each months also may the rate of people who visit the hospital to do the test , the lowest distribution to occur in July by (1.9%), on the other hand the highest distribution in March (5%) followed by January (4.3%) and February(4.3%) as shown in (Figure 2) which might be due to the seasonal change as people go outside, do outdoor activities, and meet each other more which affect the rate of transmission, and might be at the beginning and end of the year more people come to do the tests.
Our study showed difference in prevalence of Entamoeba histoytica infection in different ages, we observed the higher percentage of infection in age (16-25) was (5.5%) followed by age (46-55) which (3.3%), and the lowest percentage of infection in age (36-45) which (2.6%) which illustrated in (Table 2), our result agreement with [36].
Higher rate observed among age (16-25) largely due to lack of personal and environmental sanitation, human behavioral, ignorance of health promotion, and may be they eat a lot of outdoor food contaminated with Entamoeba histoytica [37].
Most infection in the hospitals are single infections by different protozoa, in our study among the intestinal protozoa Entamoeba histolytica, exhibited the highest rate of infection (3.6%) followed by Giardia lamblia (1.1%) as observed in (Figure 3).
These two protozoan remain the most common intestinal parasitic pathogens. Our result was close to finding in Saudia Arabia by [38], and was different from northern Jordon [39]. The presence of Entamoeba histolytica in the stool suggests the possibility of patient’s exposure to the environmental conditions that may result in ingestion of contaminated food or water containing pathogenic parasites. Also, it could be attributed to the susceptibility for infection by Entamoeba and/or the availability of the sources of infection by this parasite [40].
In conclusion, it was finalized that Entamoeba hisolytica is present particularly during cold seasons. Prevalence of amoebic infection among food handlers in Erbil city was low. Statistically significant difference was observed in infection according to gender.
References
- Stanley JrSL. Amoebiasis, the Lancet. 2003; 361(9362): 1025-1034.
- Bercu TE, Petri WA, Behm BW. Amebic colitis: New insights into pathogenesis and treatment. Current gastroenterology reports. 2007; 9(5): 429-433.
- Kumanan T, Sujanitha V, Balakumar S, Sreeharan N. Amoebic liver abscess and indigenous alcoholic beverages in the tropics. Journal of Tropical Medicine. 2018; 6: 1-2.
- Petri JrWA, Haque R, Lyerly D, Vines R. Estimating the impact of amebiasis on health. Parasitology Today. 2000; 16(8): 320-321.
- Pinilla AE, Lopez MC, Viasus DF. History of the Entamoeba histolytica protozoan. Revista medica de Chile. 2008; 136(1): 118-124.
- Haque R, Huston CD, Hughes M, Houpt E, Petri JrWA. Amebiasis. New England journal of medicine. 2003; 348(16): 1565-1573.
- Wuerz T, Kane JB, Boggild AK, Krajden S, Keystone JS, et al. A review of amoebic liver abscess for clinicians in a nonendemic setting. Canadian Journal of Gastroenterology. 2012; 26(10): 729-733.
- Cornick S, Chadee K. Entamoeba histolytica: Host parasite interactions at the colonic epithelium, Tissue Barriers. 2017; 5(1).
- Thibeaux R, Weber C, Hon C, et al. Of the Virulence Landscape Essential for Entamoeba histolytica Invasion of the Human Colon, PLoS Pathogens. 2013; 9(12): e1003824.
- Kumiko NT, Tomoyoshi N. Immune response of amebiasis and immune evasion by Entamoeba histolytica. Frontiers in immunology. 2016; 7: 175
- Misra SP, Misra V, Dwivedi M, Singh PA, Barthwal R. Factors influencing colonic involvement in patients with amebic liver abscess. Gastrointestinal endoscopy. 2004; 59(4): 512-516.
- Lodhi S, Sarwari AR, Muzammil M, Salam A, Smego RA. Features distinguishing amoebic from pyogenic liver abscess: A review of 577 adult cases, Tropical Medicine & International Health. 2004; 9(6): 718-723.
- Shamsuzzaman SM, Hashiguchi Y. Thoracic amebiasis Clinics in Chest Medicine. 2002; 23(2): 479-492.
- Nunes MC, Guimarães JMH, Diamantino AC, Gelape CL, Ferrari TC. Cardiac manifestations of parasitic diseases, Heart. 2017; 103(9): 651-658.
- Garcia LS, Arrowood M, Kokoskin E, Paltridge GP, Pillai DR, et al. Practical guidance for clinical microbiology laboratories: laboratory diagnosis of parasites from the gastrointestinal tract. Clinical microbiology reviews. 2018; 31(1): e00025-17.
- Hiatt RA, Markell EK, Ng E. How many stool examinations are necessary to detect pathogenic intestinal protozoa? The American journal of tropical medicine and hygiene. 1995; 53(1): 36-39.
- Al-Daoody AAKh, Ismail SM, Ezadin ZY, Ahmad DK. Prevalence of Giardia Lamblia among Residents of Hawler, Soran and Chamchamal Cities, North of Iraq. Pak-Euro Journal of Medical and Life Sciences. 2020; 3(2): 28-36.
- Lien, et al. Effects of the infant stool color card screening program on 5‐year outcome of biliary atresia in Taiwan. Hepatology. 2011; 53(1): 202-208.
- Kasirga E. Cocuklarda sindirim sistemi hastaliklarinin tani ve izleminde diski incelemelerinin yeri/The importance of stool tests in diagnosis and follow-up of gastrointestinal disorders in children. Turkish Pediatrics Archive. 2019; 54(3): 141-149.
- Vandenberg O, Van Laethem Y, Souayah H, Kutane WT, Van Gool T, et al. Improvement of routine diagnosis of intestinal parasites with multiple sampling and SAF- fixative in the triple-faeces-test. Acta gastro-enterologica belgica. 2006; 69(4): 361-366.
- Evangelopoulos A, Legakis N, Vakalis N. Microscopy, PCR and ELISA applied to the epidemiology of amoebiasis in Greece. Parasitology international. 2001; 50(3): 185-189.
- Yilmaz H, Abdullah A. Prevalence of Intestinal parasites (Entamoeba sp. and Giardia lamblia) in Duhok and Erbil cities. Northern Iraq. J Microbiol Exp. 2017; 4(6): 00132.
- Al-Daoody AAKh, Ali FA, Sadiq LB, Mamand AS, Rawezh Salah Ismail RS, et al. Investigation of Intestinal Protozoan Infections among Food-Handlers in Erbil City, Iraq. Plant Archives. 2021; 21(1): 1367-1372. doi.org/10.51470/.
- Stauffer, Ravdin. Entamoeba histolytica: an update. Current opinion in infectious diseases. 2003; 16(5): 479-485.
- Dafalla AIA, Almuhairi SASO, AlHosani MHJ, Mohamed MY, Alkous MIA, et al. Intestinal parasitic infections among expatriate workers in various occupations in Sharjah, United Arab Emirates. Revista do Instituto de Medicina Tropical de São Paulo. 2017; 59.
- Al Alkeem F, Loney T, Aziz F, Blair I, Sonnevend Á, Sheek-Hussein M. Prevalence and factors associated with infectious intestinal diseases in Ras Al Khaimah, United Arab Emirates, 2017: A population-based cross-sectional study. International Journal of Infectious Diseases. 2019; 85: 188-194.
- Shobha M, Bithika D, Bhavesh S. The prevalence of intestinal parasitic infections in the urban slums of a city in Western India. Journal of infection and public health. 2013; 6(2): 142- 149.
- Okyay P, Ertug S, Gultekin B, Onen O, Beser E. Intestinal parasites prevalence and related factors in school children, a western city sample-Turkey. BMC public health. 2004; 4(1): 1-6.
- Dhubyan MZ. Prevalence of Entamoeba histolytica and Giardia Lamblia Associated with Diarrhea in Children referring to lbn Al-Atheer Hospital in Mosul, Iraq. Archives of Razi Institute. 2022; 77(1): 73-79.
- Damen JG, Cosmas EU and Damak CA. Intestinal Parasitosis among Food Handlers in Jos, North Central Nigeria. Danish Journal of Agriculture and Animal Sciences. 2015; 2: 53-58.
- Amer OS, Al-Malki ES, Waly MI, AlAgeel A, Lubbad MY. Prevalence of intestinal parasitic infections among patients of King Fahd Medical city in Riyadh region, Saudi Arabia: a 5-year retrospective study. Journal of parasitology research. 2018; 8: 2-5.
- Hussein RA, Shaker MJ, Majeed HA. Prevalence of intestinal parasitic infections among children in Baghdad City. Journal of College of Basic Education. 2011; 71: 130-147
- AL-Shaheen, Kassim AL-Maki, Khalaf. A study on prevalence of Entamoeba histolytica & Giardia Lamblia infection. Basrah Journal of Veterinary Research. 2007; 6(2): 30-36.
- Maharana BR, Kumar B, Sudhakar NR, Behera SK, Patbandha TK. Prevalence of gastrointestinal parasites in bovines in and around Junagadh (Gujarat). Journal of parasitic diseases. 2016; 40(4): 1174-1178.
- AlAyyar RM, AlAqeel AA, AlAwadhi MS. Prevalence of Giardiasis and Entamoeba Species in Two of the Six Governorates of Kuwait. Journal of Parasitology Research. 2022; 6(2): 2-3.
- Faraj A, Koyee Q. Epidemiology of intestinal parasites among food handlers in Erbil city. Duhok Medical Journal. 2012; 6(1): 1-12.
- Gholipoor Z, Khazan H, Azargashb E, Reza Youssefi M, Rostami A. Prevalence and risk of intestinal parasite infection in Mazandaran province, North of Iran. 2020; 8(1): 17-20.
- Amer OH, Ashankyty IM, Haouas NAS. Prevalence of intestinal parasite infections among patients in local public hospitals of Hail, Northwestern Saudi Arabia. Asian Pacific journal of tropical medicine. 2016; 9(1): 44-48.
- Jaran AS. Prevalence and seasonal variation of human intestinal parasites in patients attending hospital with abdominal symptoms in northern Jordan. EMHJ-Eastern Mediterranean Health Journal. 2016; 22(10): 756-760.
- Bayoumi, et al. Intestinal parasitic infections in school students in Malakal city, Upper Nile State, South Sudan. SOJ Microbiol Inf Dis. 2016; 4(1): 1-5.