
SciBase Journals
SciBase Neurology
ISSN 2996-3788
- Article Type: Commentary
- Volume 2, Issue 3
- Received: Mar 20, 2024
- Accepted: Apr 23, 2024
- Published Online: Apr 30, 2024
Safety of Three Level Cages used without Plate Fixation in Anterior Cervical Discectomy
Khalid Bin Madhi*
Kasr Alainy Medical School, Cairo University, Cairo, Egypt.
*Corresponding Author: Khalid Bin Madhi
Kasr Alainy Medical School, Cairo University, Cairo, Egypt.
Email: karimeldabaa@yahoo.com
Citation: Madhi KB. Safety of Three Level Cages used without Plate Fixation in Anterior Cervical Discectomy. SciBase Neurol. 2024; 2(3): 1023.
Introduction
Cervical Spondylotic Myelopathy (CSM) is common clinical disease [1]. Anterior cervical discectomy and fusion for treatment of CSM was firstly introduced by Simth, Robinson and Cloward, the anterior procedure had become the most widely used surgical choice [2].
Anterior approach allows direct decompression of spinal cord and uses of Three level cage without plate fixation is safely and effective [3].
Anterior cervical discectomy and fusion has been considered the gold standard surgical procedure for Treatment of degenerative cervical spinal disease.
Objective
The aim of surgery is to decompress spinal cord and evaluate safety of Three level cage used without plate fixation to preserve the stability of spinal column.
Patient and methods
This study include 40 patients underwent for surgery ((ACDF)) with cages for degenerative cervical disc disease affection three level from 2015-2023.
PEEK cages were used in all cases and follow up for one year.
The mean age for these patients was (57 yrs) ranged (45-70 yrs).
The Indication for surgery was progressive myelopathy resulting from degenerative cervical disease, which it failed for medical treatment.
Surgical technique
All patients underwent for general anesthesia, on supine position with mild neck extension right side approach was performed via T-shape incision, platysma was elevated by small curved forceps then cutting, omohyoid muscle also cut, then identify important structure carotid sheet laterally and thyroid, trachea medially, pre vertebral fascia and longus colli muscles were mobilized, the operative level confirmed by fluoroscopy x-ray.
Caspar pins was used for distraction, then distraction was done, started from superior level, down word to last one.
In all cases posterior longitudinal ligament was cutting, also foraminotomies done.
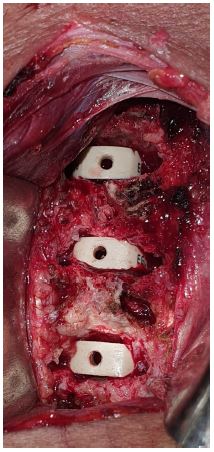
After suring of decompression for spinal cord, the proper size of PEEK cage is insertion to inter-vertebral space, confirmed by the x-ray.
Assessment of patients
All patients were assessed clinically and radiologically preoperative- Immediately post-operative and follow up at 3, 6 month post-surgery we are selected result at 3 month follow up to compare between two group pre & post-operative follow up in VAS, Cobb angle, disc height.
Results
No= 40 patient; Age range 45-70 years
| Age | No. pt |
|---|---|
| 45-54 | 5 |
| 55-64 | 10 |
| 65-70 | 25 |
| Femals | Male |
|---|---|
| 5 | 35 |
| 12.5% | 87.5% |
| Clinical presentation | No. pt. | Percentage |
|---|---|---|
| Myelopathy + radiculopathy | 30 | 75% |
| Myelopathy | 10 | 25% |
| Complication | No. Pt | % |
|---|---|---|
| Temporary dysphagia | 5 | 12.5 |
| Dura tear | 1 | 2.5 |
| Infection | - | - |
| Pseudoarthrosis | 3 | 7.5 |
| Subsidence | 3 | 7.5 |
| Weakness | 1 | 2.5 |
| The improvement | ||
|---|---|---|
| Excellent | 15 | 37.5% |
| Good | 20 | 50% |
| Fair | 5 | 12.5% |
| Poor | - | 0% |
Clinical and radiological assessment of patient
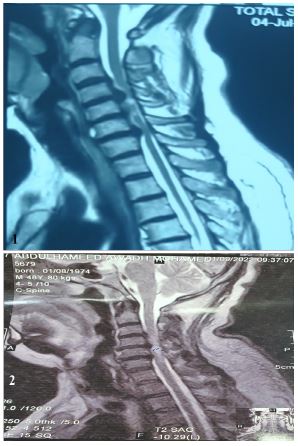
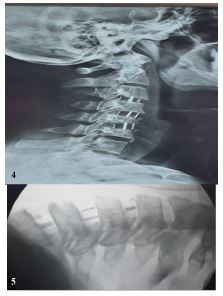
Radiological assessment used MRI to identify discs herniation and sign of myelopathy is very important, but plain radiographs in lateral and dynamic view are other parameters for assess (fusion rate, intervertebral height, cervical lordosis with using the cobb angle and present solid arthrodesis or pseudoarthrosis).
Odom’s criteria was used for post-operative assessment.
Odom’s criteria (Figure 3)
| Definition | Grade |
|---|---|
| All preoperative symptoms relieved, able to carry out daily occupation without impairment. | Excellent |
| Minimum persistence of preoperative symptoms, able to carry out daily occupation without significant interference. | Good |
| Relief of some preoperative symptoms, but whose physical activities were significant limited. | Fair |
| Symptoms and signs unchanged or worse. | Poor |
The mean of cobb angle pre-operative was 10 which was decrease to 3 post-operative group while the mean of disc height was 3.25 mm in pre-operative improve to 5.5 mm in post-operative group in (92.5%).
The clinical follow up were assessed by comparing the scores on 10 point visual analogue scale neck pain and arm pain in tow group pre-operative and post-operative, were recorded the mean of neck pain and arm pain (6, 5.75 respectively) in pre-operative group.
The mean of VAS was 5.87 in first group which was decrease in post-operative group to 2.49.
This result according to selection of follow up at 3 month post-operative where the mean of neck pain was 2.87 while the mean of arm pain was 2.12.
Discussion
Complication
The most common complication post-operative was transient dysphagia which observed in (12.5%) of all patients, this result is nearly percentage described by M. Ajello et al. V58-suppl to NO2, 2014 which was (9.5%) [4].
The weakness was other complication happen in one case represent (2.5%) in the form of immediate post-operative Paraparesis, grade 2 weakness of both lower limb, this weakness improved during first week of post-operative period, this was agree with study of yonenobu et al. report (3.4%) of post-operative [5].
Radiological finding in this study regarding to fusion, it was good in all cases, then the mean of cobb angle in this study was 10 degree pre-operative which decrease to 3 degree post-operative while the mean of disc height was 3.25 mm in preoperative group improved to 5.5 mm in post-operative group in percentage (92.5%) in 3 month follow up with 3 case subsidence in (7.5%) as complication in our study, which was increase than study of Hamgliu [6], report on case subsidence in (4%) while study of Hwang et al. report (6.3%) of cage subsidence [7].
We report 3 cases had pseudoarthrosis represent (7.5%) in compare with study of Papadopoulos et al. [8]. There was 2 case pseudoarthrosis of their 46 cases.
The aim of this study was to prove the radiological finding and clinical follow up to assisted anterior cervical discectomy and fusion on patients for three levels use cages without plating [9].
The mean age was 57 yrs, this nearly of study of Osama M abdelwahab et al volume 29/No.3/July 2014 53-58 [10].
But the percentage of male more than female, which was 87.5% male to 12.5% female.
The main clinical presentation was neck pain and arm pain
The mean of neck pain and arm pain was (6, 5.7 respectively) in pre-operative group, where decrease in post-operative group to (2.87 and 2.12) in three month follow up postoperative, but the mean of VAS was 5.87 in preoperative group which was decrease to 2.49 in post-operative group, these result in this study agree with study of liu et al. [11].
References
- Yalmanchili PK, Vives MJ, Chaudhary SB. cervical spondylotic myelopathy: Factors choosing the surgical approach.Advances in orthopedics. 2012; 783762.
- Cloward RB. The anterior approach for removal of rupture cervical discs. Journal of neurosurgery. 2007; 6: 496-511.
- Cbraja M, Abbushi A, Koeppen D, Kroppenstedt S. Woiciechowskyc J. Comparison between anterior and posterior decompressionwith instrumentation for cervical spondylotic myelopathy: Saggital alignment and cervical clinical outcome. Nweosurg. Focus. 2010; 20(3): E15.doi:10.3171/2010.1. Focus 09253.
- M Ajello, et al. 2014; 58(2).
- Yonenobu K, Honson N, Iwasaki M, Asamo M. Neurologic complications of surgery for cervical compression myelopathy. Spine. 1991; 16: 1277-82.
- Hngliu, Avraam Ploumis, Chundle Li, Xiaodong Yi, Hong Li. Polyetheretherketone cages Alone with ALLograft for three level anterior cervical fusion. ISRN Neurology. 2012; 452703.
- Hwang SL, Lin CL, Lieu As, et al. Three level and four level anterior cervical discectomies and titanium cage-augmented fusion with and without plate fixation. Journal of neurosurgery. 2004; 1(2): 160-167.
- Papadopoulos EC, Huang RC, Giradi FP, Synnottk, Cammisa FP. Three level anterior cervical discectomy and fusion with plate fixation: Discectomy and fusion with plate fixation: radiographic and clinical results. Spine. 2006; 8: 897-902.
- Chody, Lee Wy. Sheupc: Treatment of multi-level cervical fusion with cages. Surgical neurology. 2004; 62(5): 378-385.
- Osama M Abdelwahab etal, Egyptian Journal of neurosurgery. 2014; 29: 53-58.
- Lie HP, Locumis A, Lic Y, Li H. polyetheretherketone cages alone with allograft for three level anterior cervical fusion ISRN Neurlogy. 2012: 5.