SciBase Journals
SciBase Oncology
- Article Type: Research Article
- Volume 2, Issue 1
- Received: Jun 12, 2024
- Accepted: Aug 14, 2024
- Published Online: Aug 21, 2024
Analysis of Ageism in Radiotherapy Oncology Group
Francesco Tramacere1*; Marzia Borgia1; Tiziana Proto1; Alessandra Sallustio1; Francesca Pati1; Maurizio Portaluri1; Salvatore Parisi2; Angelo Errico3; Girolamo Spagnoletti4; Anna Rita Marsella5; Cristina Barba6; Maria Paola Ciliberti7; Sabino Bonaduce8; Angela Sardaro9; Grazia Lazzari10; Alessandra Castelluccia1
1Radioterapia, ASLBR Ospedale “A. Perrino” Brindisi, Brindisi, Italy.
2Radioterapia Oncologica IRCCS Casa Sollievo della Sofferenza S. Giovanni Rotondo, Italy.
3Radioterapia P.O. “R. Dimiccoli” ASLBT Barletta, Italy.
4Radioterapia Policlinico di Foggia, Italy.
5Radioterapia Oncologica P.O. “S.G. Moscati” Taranto, Italy.
6Radioterapia Ospedale Vito Fazzi Lecce, Italy.
7Radioterapia Ospedale Generale Regionale “F. Miulli” Acquaviva delle Fonti, Italy.
8Radioterapia IRCCS Giovanni Paolo II Bari, Italy.
9Radioterapia Azienda Ospedaliero Universitaria Consorziale Policlinico di Bari, Italy.
10Radioterapia Oncologica IRCCS CROB Rionero in Vulture, Italy.
*Corresponding Author: Francesco Tramacere
Radiotherapy Unit, “A. Perrino” Hospital, Strada Statale 7 Per Mesagne, 72100 Brindisi, Italy.
Email: francesco.tramacere@asl.brindisi.it
Abstract
We tried to investigate any discriminatory attitudes towards elderly people through the administration of questionnaires to all healthcare workers in 10 radiotherapy oncology departments in the regions of Puglia and Basilicata. Some ageist attitudes have emerged; not as discriminatory acts but as the result of archaic, unconscious and stereotyped conceptions. The age problem is mainly due to false information that causes misconceptions about the elderly.
Citation: Tramacere F, Borgia M, Proto T, Sallustio A, Pati F, et al. Analysis of Ageism in Radiotherapy Oncology Group. SciBase Oncol. 2024; 2(1): 1014.
Introduction
Europe’s population is ageing. The share of elderly people (over 65) in the European population went from 16% in 2001 to 21% in 2020 (23% in Italy) [1]. Thanks to the increase in survival from the post-war period to today. This increase in life expectancy, resulting from improvements in the quality of life and advances in medicine, leads to an increase in demands for healthcare [2]. This, in turn, also leads to a series of changes related to the needs of the elderly, to the behaviours and attitudes of the rest of the population towards them and can lead to acts of discrimination against this part of the population. The World Health Organization’s global report (WHO) Age Discrimination refers to stereotypes (how we think), prejudices (how we feel), and discrimination (how we act) against others or oneself based on age. Globally, one in two people are ageist against older people. In Europe, the only region for which we have data, one in three report having been a target of ageism, and younger people report more perceived age discrimination than other age groups [3]. The impact of ageism has serious and far- reaching consequences for people’s health, well-being and human rights [4]. For older people, ageism is associated with a shorter lifespan, poorer physical and mental health, slower recovery from disability and cognitive decline [5]. Ageism reduces older people’s quality of life, increases their social isolation and loneliness (both of which are associated with serious health problems), restricts their ability to express their sexuality and may increase the risk of violence and abuse against older people [6]. Robert Butler first defined “the systemic maintenance of stereotypes and discrimination against people because of their age” with the concept of ageism [7]. Although he identified negative attitudes (e.g., disease, incapacity, ugliness, strain in mental functions, mental illness, uselessness, isolation, poverty, and depression) argued that ageism also covers positive attitudes (e.g., compassion, wisdom, trustworthiness, political power, freedom, and happiness) [2]. However, negative aspects of ageism are generally constituted by de-individualising and devaluing older persons through particular attitudes, practices and culture [8]. Ageism pervades many institutions and sectors of society, including work, the media, justice and healthcare. Age-based rationing of healthcare is widespread and older people tend to be excluded from research and data collection activities [4]. COVID-19 has affected people of all ages, in different ways. But beyond the impacts of the virus itself, some of the narratives about different age groups have exposed a deep and older malady: ageism. Older people have been often seen as uniformly frail and vulnerable, while younger people have been portrayed as invincible, or as reckless and irresponsible. Another aspect of age discrimination relates to the way health care providers communicate with older adults. A number of studies provide evidence that patronizing and ineffective communication can characterize discourse between providers and older patients [8]. Discrimination based on age may be reflected in clinical practice and decision making among health care providers. Studies using both hypothetical decision making scenarios and patient record review have demonstrated age-based disparities in diagnostic procedures as well as in the types of treatment offered to patients. These reports emerge from various fields of medicine including the oncology [8]. Approximately 64% of new cancer cases registered every year in Italy affect people over 65 years of age [9]. A cancer diagnosis is a potentially traumatic event in a person’s life, and can be particularly traumatic for an elderly person. Furthermore, around the concept of cancer there are beliefs, even wrong ones, which seem to be rooted especially in people of a certain age. To these beliefs we can add the ageist attitudes of healthcare workers which could be even more dangerous in the oncology field.
Oncology today involves the collaboration of a multidisciplinary group. Together with surgery and chemotherapy, radiotherapy represents a fundamental weapon in the fight against cancer. It uses highly energetic ionizing radiation aimed at the neoplastic mass for treatment. The radiotherapy department is a different environment from an inpatient department and different from a radiology service. Most treatments take place on an outpatient basis with daily and repeated access for several days (from 1-5 to over 30-40 days). Like the personal beliefs of a group of healthcare professionals in the field of radiation oncology, they can emerge in one of the most important healthcare activities of personal care and assistance. The aim of this work is to investigate these aspects in the radiation oncology department. In particular, if there are ageist attitudes of operators towards elderly patients, what nature they are, who commits them and the possible solutions.
Materials and methods
A total of 174 radiotherapy oncology healthcare providers (radiation oncologists, nurses, physics, radiation technologists and social workers) with median age 47 years (range 23-70, mean 45) who was administered a questionnaire compiled between June 2022 and january 2023 in 9 radiotherapy departments in Puglia and Basilicata regions (Acquaviva Delle Fonti, Barletta, Bari, Brindisi, Foggia, Lecce, Rionero in Vulture, SG Rotondo and Taranto) which are part of the regional AIRO group (Associazione Italiana Radioterapia Oncologica). The questionnaire was completed anonymously. Each questionnaire was made up of 30 questions divided into 5 groups:
Group 1: 6 questions on personal details and cohabitation
Group 2: 6 questions investigating aspects of separation and avoidance Group 3: 7 questions that investigated aspects of stereotypes and clichés.
Group 4: 5 questions investigating aspects of negative emotions and discrimination Group 5: 6 questions investigating specific aspects of the radiotherapy field.
The questionnaire is similar to the one validated by the University of Bari [10] with the aim of investigating the prejudices of psychologists during their professional activity towards elderly subjects, modified to be oriented towards the radio-oncology field.
The questions of the 1st group concerned information on age, sex, marital status, children, cohabitants and presence of elderly people. The questions of the 2nd group concerned information to highlight whether there are attempts to avoid contact with the elderly patient and raise a separation barrier. The questions of the 3rd group concerned information to understand if the operator is a victim of clichés and stereotypes such as that the elderly person is oriented towards looking at the past, is closed to the new, is stingy and pays little attention to personal hygiene. The questions in the 4th group concern prejudices which, if expressed in negative terms, fuel discriminatory attitudes. The questions of the 5th group concerned specific information about the radiotherapy treatment on the time and methods of execution.
The literature contains various scales developed to measure ageist discrimination. Scales containing cognitive, emotional, and behavioral dimensions are limited. The Fraboni Scale of Ageim (FSA) contains these three dimensions. The FSA measures the attitudes of young toward older, and examines these attitudes not as a single characteristic, but as a combination of the elements of avoidance and discrimination [7].
Results
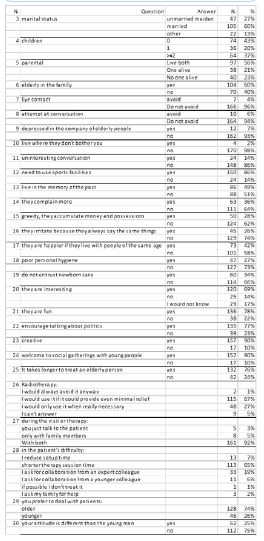
The respondents were 64% women and 36% men. Almost half of the professionals surveyed were relatively young (median 47). Of these professionals, more than half (60%) had experience with older people. Another important piece of information for understanding the sample concerns the marital status of the respondents: 60% were in a romantic relationship, cohabiting or married, while 27% were single, 13% were separated, divorced or had lost their partner (Table 1).
Also significant is the fact that for 56% of respondents both parents were still alive, for 21% only one of the two parents was still alive, while 23% had lost both. The questions from group 2 show that only 4% rarely avoid eye contact with older people and 10% say that they do not like talking to them [11]. Almost 7% say that they often feel depressed around older people. Only 4% believe that older people should live where they do not disturb anyone. 14% believe that you cannot expect complex and interesting conversations from older people. Only 14% believe that older people do not necessarily need to use the city’s sports facilities (Table 1). In Group 3, over 50% believe that many older people only live in memories of the past. Almost 36% believe that older people complain much more and to a greater extent than other people. 28% believe that older people are greedy and hoard money and possessions. Almost 26% believe that older people can be annoying because they repeat the same things over and over again. 42% believe that older people are happier when they are with their peers. 27% believe that most older adults pay little attention to their personal hygiene. 34% believe that older people should not be trusted with newborn babies (Table 1). In group 4, 14% believe that older people are uninteresting. 22% of respondents believe that older people are not fun to date. Almost 23% do not believe that older adults should be encouraged to talk about politics. 17% do not believe that older people can be very creative. 17% do not believe that older people should participate in social gatherings with younger people (Table 1). In group 5, 76% believe that it takes longer to treat an elderly patient. 67% believe that radiotherapy should only be used if it can provide even minimal relief, and 27% only in really necessary cases. 92% would talk to both the patient and the family member during the visit or treatment. In case of difficulties in carrying out the treatment, they would shorten the duration of the session and in 19% of cases they would ask professional colleagues for help. 74% did not prefer to work with younger or older patients. Also, when asked whether the attitude towards an older patient differs from that towards a young one, 75% answered that it does not differ, and at the same time this percentage did not change depending on the age of the practitioner.
Table 1: Questionnaire answers.
Discussion
Recent research [12] raises the question of the links between ageism and health problems and points the way forward against ageism as a strategy for the health and well-being of older adults. The authors of a review came to the same conclusions [13,14]. These statements appear to be even more relevant to the field of oncology. The FSA states that ageism has three dimensions: cognitive, emotional and behavioral. These three dimensions can relate to oneself or to others (both in institutions and in relationships) on the basis of age and can be positive or negative, conscious or unconscious [2].
The sample of respondents in our adaptation of the Italian validation of the FSA showed a discontinuous tendency of ageism (sometimes present, sometimes almost absent), but ageism did not prove to be a widespread phenomenon of ghettoization, as it manifests itself mainly at the level of prejudice against older people [2].
It is precisely in group 2, referring to stereotypes and clichés, that the largest percentage of ageist responses was found, dictated by a persistent, normalizing and socially accepted tendency of society towards incorrect linguistic and social practices corresponding to antilocution, i.e. a general aversion based on misunderstanding and misinformation.
However, the radiotherapy staff seemed calm and open to dialog. Often a relationship of trust and friendship is also established through the long duration of therapy. The presence of optimization forms, often combined with requests for help in finding the simplest possible alternative solutions, was one of the strategies used, as was seeking the cooperation of family members wherever possible, which instilled confidence and a sense of serenity in the patient and dispelled some ageist attitudes that tended to emerge not as discriminatory acts but as a result of archaic, unconscious and stereotypical ideas. An important fact is that in 25% of the cases there is a different attitude towards young people and in 26% of the cases there is a preference for young people. The preference for dealing with younger patients is not due to ageist behavior, but probably to mere professional preferences dictated by previous professional experience. Respect for the dignity of the person was never questioned and not only expressed, but is deeply rooted in the daily lives of the operators interviewed.
From the results of the 4th group, we can conclude a protectionist bias and no form of discrimination against older people and pay great attention to both informed consent and privacy policies, as well as the empathetic and humanizing aspect of care. This finding also confirms that focusing on empathy as a privileged tool for appropriate information sharing and changing the discussion about aging is an important first step in changing the reality and also the perception of reality for people over 65. Therefore, society is called to refine generalist statements and utilize new discursive strategies to combat the common notion of a ‘separate group’ and move beyond fixed age identity categories; to view aging less categorically with different and ever-evolving needs and interests; and to narrow the “gap’ between generations [2].
According to a study by the Center of Social Investment Studies (Centro Studi Investimenti Sociali, Censis), 49.3% of “millennials” (those born between 1980 and 1995) in Italy think it is right to prioritize young people in emergency situations, while 35% believe that the proportion of public spending on older people is too high (55th Censis Report). It cannot therefore be ruled out that the attention paid to older people in recent months following the pandemic has led to some anger among young people and the most neglected social groups, reinforcing certain stereotypical attitudes.
The central role played by knowledge about the aging process is evident from the results of the questionnaire. Knowledge has a negative influence on both fear of aging and stereotypical attitudes towards older people. It is therefore confirmed that greater knowledge about aging predicts both a lower fear of aging and a more positive attitude towards older people. Fear of aging is then a predictor of stereotypical attitudes towards older people, which in turn are a positive predictor of ageism, both directly and in the role of mediating the relationship between fear of aging and ageism, as they help to construct meaning and interpretations of the world and guide the everyday actions of society. To neutralize the effects of ageist attitudes among health professionals in the treatment of older people, we sought to raise awareness of ageism among 174 health professionals in radiation oncology by presenting and evaluating the questionnaire to address a problem that is present in society and affects an important segment of the population. Just by using the questionnaire, their awareness of ageist attitudes was raised, which at other times might have lain dormant and attracted negative attention [2].
ConclusionConclusion
The recommendation for further research is to investigate aging behavior and the factors that influence this behavior in a larger sample group and in different occupational groups working in healthcare [2].
Although this research finding is limited due to the small sample size, it can serve as an indicator of where the problem lies (misinformation leading to misconceptions about older people) [2].
Therefore, our hypothesis is that this dimension of ageism can be almost radically addressed and neutralized if we invest in the training of new health professionals who can provide direct access to appropriate information about the health assessment and treatment of older people, as well as support increased professional development, educational opportunities, and further scientific research [2].
References
- Rapporto annuale Istat. 2 How mental health professionals perceive old(er) adults: Findings from an ageism scale used for. 2019. https://www.istat.it/storage/rapporto-annuale/2019/Sintesi2019.pdf
- Discourse analysis purposes. Journal of language and discrimination. Rosita Maglie; Ignazio Grattagliano. 2022. doi: 10.1558/jld.21298.
- Portuguese Version of the Ageing Attitudes Questionnaire (AAQ): Validation of the Psychometric Properties. Margarida Pedroso de Lima, Paulo Martins, António-José Gonzalez; Int J Environ Res Public Health. 2022; 19(24): 16778.
- Reducing the Burden of Ageism, Mentalism, and Ableism: Transforming the Narrative for Older Persons with Mental Health Conditions and Psychosocial Disability.
- Quinn G, Mahler C. Am J Geriatr Psychiatry. 2021; 29(10): 993-994. Epub 2021 May 26.
- S Brink. Springer The Longevity Dividend. https://link.springer.com: Book. 2023.
- Global report on ageism: https://www.who.int/publications/i/item/9789240016866.
- Irem Ozel Bilim, F Yasemin Kutlu.. The psychometric properties, confirmatory factor analysis, and cut-off value for the Fraboni scale of ageism (FSA) in a sampling of healthcare workers. Perspect Psychiatr Care. 2021; 57(1): 9-19.
- Liat Ayalon, Clemens Tesch-Romer. Contemporary perspectives on Ageism. Springer Open. 2018 ; 2-3..
- https://www.registri-tumori.it/PDF/AIOM2016/I_numeri_del_cancro_2016.pdf 10 survey site uniba: https://forms.gle/aRfn9JxptXopCHkw5.
- Somkiat Eiamkanchanalai, Nuttapol Assarut, Suwanee Surasiengsunk. Attitude toward the elderly and social interaction: Approach toward an intergenerational society.. Kasetsart Journal - Social Sciences. 2019; 40(3).
- Julie Ober Allen, et al. Geriatrics Experiences of Everyday Ageism and the Health of Older US Adults. JAMA Network Open. 2022; 5(6): e2217240. doi:10.1001/jamanetworkopen.2022.17240.
- E-Shien Chang, et al: Global reach of ageism on older persons’ health: A systematic review PLOS ONE. 2020. https://doi.org/10.1371/journal.pone.0220857 January 15, 2020.
- Anat Shoshani, Ariel Kor. The longitudinal impact of the COVID-19 pandemic on adolescents’ internalizing symptoms, substance use, and digital media use. Eur Child Adolesc Psychiatry. 2023.
Supplementary data
Research questionnaire on the ageism of radiotherapy oncology operators
1) Age
2) Gender: Woman Man
3) Marital status: Single Married Separated Divorced Widowed Other
4) Do you have children? If yes, how many?
5) Are her parents alive? Yes, both. No, neither of them. Only one of the two
6) Are there elderly people in your family? Yes No
7) I sometimes avoid eye contact with older people when I see them. Yes No
8) I don’t like it when an elderly person tries to make conversation with me. Yes No
9) Feeling depressed is a common feeling when in the company of elderly people. Yes No
10) Meglio che le persone anziane vivano dove non infastidiscono nessuno/a.Si No
11) You cannot expect a complex and interesting conversation from most older people. Yes No
12) Older people don’t really need to use our municipal sports facilities. Yes No
13) Many elderly people have been living only in the memory of the past for years. Yes No
14) Elderly people complain more than other people. Yes No
15) Many elderly people are miserly and accumulate money and possessions. Yes No
16) Most older people can be irritating because they always tell the same stories. Yes No
17) Many older people are happier when they are with people of their own age. Yes No
18) It is claimed that most elderly people have poor personal hygiene. Yes No
19) Most elderly people should not be entrusted with the care of newborns. Yes No
20) Most older people are interesting. Yes No
21) The company of most older people is quite fun. Yes No
22) Older people should be encouraged to talk openly about politics. Yes No
23) Older people can be very creative. Yes No
24) Older people should be welcome at social gatherings of younger people. Yes No
25) It takes longer to treat an elderly patient. Yes No
26) What do you think, beyond the guidelines, about the use of radiotherapy in very elderly patients? a) I would always avoid it anyway. b) I would use it if it could provide even minimal relief. c) I would only use it in truly necessary cases. d) I can’t answer beyond the guidelines
27) When you accept, take a medical history, visit or treat a very elderly patient capable of understanding, address all possible discussions, interactions and make any indications with: a) only the patient’s family members. b) only with the elderly patient. c) both
28) In the inability or impossibility of the elderly patient to make decisions regarding her health; a) I reduce the set up reproduction time. b) I apply as little time as possible to the entire session, in the right way. c) I always ask a more experienced colleague for help. d) I ask for collaboration from a younger colleague. e) if possible I avoid treating it myself.
29) Generally speaking, do you prefer dealing with younger patients (<70 years old)?
30) Is your attitude different with an elderly patient than with a young one (<40 years)?.