SciBase Journals
SciBase Oncology
- Article Type: Research Article
- Volume 2, Issue 3
- Received: Aug 30, 2024
- Accepted: Oct 09, 2024
- Published Online: Oct 16, 2024
Lineage-Specific Mixed Chimerism in Pediatric Allogeneic Hematopoietic Stem Cell Transplantation for Acute Myeloid Leukemia
Saadiya Khan1; Ibrahim Jafaari2; Khawar Siddiqui1*; Hawazen AlSaedi1; Ali Al-Ahmari1; Abdullah Al-Jefri1; Ibrahim Ghemlas1; Awatif AlAnazi1; Mouhab Ayas1
1Department of Pediatric Hematology/Oncology, King Faisal Specialist Hospital and Research Center, Riyadh, Saudi Arabia.
2Department of Pediatric Hematology/Oncology, Prince Mohammed Bin Nasser Hospital Jazan, Saudi Arabia.
*Corresponding Author: Khawar Siddiqui
Department of Pediatric Hematology/Oncology, King Faisal Specialist Hospital and Research Center, Riyadh, Saudi Arabia.
Tel: +966-11-205-5278;
Email: ksiddiqui@kfshrc.edu.sa
Abstract
Hematopoietic Stem Cell Transplantation (HSCT) is considered a curative option for children with Acute Myeloid Leukemia (AML). Post-HSCT relapse in pediatric AML is associated with poor outcomes. Our ability to predict this event is limited. Chimerism analysis can be followed sequentially to detect Mixed Chimerism (MC) trends to identify the risk of relapse. We reviewed our data on lymphoid MC in pediatric patients with AML post-HSCT to investigate its significance as a predictor of relapse of primary disease and survival. Twenty-eight HSCT recipients fared beyond Day+120 and were the focus of this report. Post-transplant ANC recovery was observed in all cases with a median of 16 days in BM/PBSC and 22 days in transplants with CB. Platelet recovery was noted in 27 with a median of 29 days in BM/PBSC and 69 days in CB. The rate of post-HCT relapse of primary disease or progression was 7.1%. Rate of post-HSCT MC from day+30 till day+100 was 50.0%, day+100 to last contact 28.0% and day+30 through last contact was 53.6%. The cumulative probability of overall survival of our cohort was 78.0%±8.0%. MC was not found to be significantly associated with post-HSCT relapse of primary disease, mortality rate, or overall survival.
Keywords: Mixed chimerism; Stem cell transplantation; Pediatric; Acute myeloid leukemia; Outcome.
Abbreviations: MC: Mixed Chimerism; HSCT: Hematopoietic Stem Cell Transplantation; PBS: Peripheral Blood Stem Cells; GVL: Graft versus leukemia.
Citation: Aleksandar E, Katerina T, Aleksandar P, Zlatko J, Nikola V, et al. Association of CCNG1 and FDXR Gene Expression during Radiotherapy with Disease- And Therapy-Related Confounding Factors in Breast Cancer Patients. SciBase Oncol. 2023; 1(1): 1001
Introduction
Pediatric Acute Myeloid Leukemia (AML) subtype accounts for 15%-20% of acute leukemias, which themselves represent about one‐third of all childhood cancers [1]. Outcomes have improved due to refined risk‐adapted chemotherapy regimens and better supportive care but still 25% of children and adolescents with AML undergo disease relapse [2-4]. Disease relapse remains a major cause of treatment failure in patients receiving allogeneic HSCT for high-risk AML Clinical prognosis for such patients remains dismal with a 2-year post relapse survival of less than 20% [6]. Early detection of AML relapse post HSCT is thus critical to ensure that disease burden is minimal and subsequently amenable to second line intervention. Posttransplant chimerism on peripheral blood samples has been used as a surrogate for monitoring disease relapse to initiate additional immunomodulatory therapies [7,8]. Chimerism can indirectly screen an impending risk of relapse while MRD allows for confirmation of leukemia. Our ability to predict relapse risk on Chimerism profile is still limited [9]. In this retrospective analysis, we reviewed our Short Tandem Repeat (STR) chimerism data to study its ability in detecting leukemia before an overt relapse.
Patients and methods
From January 2012 to December 2017, 53 pediatric AML patients (age ≤14 years at infusion) underwent allogeneic blood and marrow transplantation at our center. Thirty-eight (71.7%) were transplant naïve and 28 (73.7%) of them fared beyond Day+120; who are the focus of this report. Detailed patient and transplant related parameters are listed in Table 1. All patients were conditioned with myeloablative regimens. Radiation was part of the conditioning regimen in 2 (7.1%) recipients only. Bone marrow was the source of stem cells in 20 (71.4%) cases. Donor was a full matched relative in 16 (57.1%), Haploidentical family member in five (17.9%) while unrelated HLA 1- or 2-AG mismatched in the remaining seven (25%) recipients who were transplanted with CB. Quantitative increase of lymphocyte Mixed Chimerism (MC) was defined as >5.0% of recipient’s DNA spiking any time during post-HCT follow-up at/beyond day+30. Graft failure and death from all causes was considered as an event. Overall survival was taken from infusion to the expiry or the last contact date, with death from any cause as an event. Chi square test or Fisher’s Exact test was employed to test the significance of association between categorical variables. Kaplan-Meier curves were drawn for survival analyses. IBM-SPSS for Windows (version 20.0) was used for statistical analysis of the data. This study was submitted to the Institutional Review Board of King Faisal Specialist Hospital and Research Center, Riyadh, Saudi Arabia, before initiation and was approved by the Research Advisory Committee through established procedures via Approval Number 2211058.
Results
Median age at HSCT was 6.9 years (range, 0.1-13.7 years). Seventeen patients (60.7%) had matched donor-recipient gender. Transplant related parameters for the cohort are provided in Table 1. Median follow-up time was 67.0±2.9 months (95% Confidence Interval: 61.2-72.8 months).
Mixed lymphocyte quantitative chimerism
Rate of lineage-specific mixed chimerism (MC) was defined as >5.0% of recipient’s DNA spiking any time during post-HCT follow-up at/beyond Day+30. MC was seen in 50% (14 out of 28 recipients) till day+100, then dropped to 25% (7 out of 25 recipients) from day+100 till last follow-up. Overall MC was 53.6% (15 out of 28 recipients) throughout follow-up till 5 years post-infusion, where applicable (Figure 1).
Graft versus Host disease
Cumulative incidence of all grade overall acute GvHD was 28.6% (n=8) whereas grade I-II acute GvHD accounted for 21.4% (n=6) and severe acute GvHD (grade III, gut) was seen in only two cases (7.1%). All grade overall acute GvHD was not found to be associated with MC (P=0.091). None of our patients exhibited chronic GvHD.
Survival, mortality and causes of death
With a mortality rate of 21.4% (n=6) and a median follow-up of 67 months (95% CI: 61.2-72.8) all survivors were in remission and clinically asymptomatic at the last contact. The cumulative probability of five-year Overall Survival (OS) and Event-Free Survival (EFS) was 78.0% (±8.0%). No statistically significant difference was found for OS or EFS for MC (≤ 5.0% vs. > 5.0%, Table 1, P=0.361). No significant association between MC and relapse of primary disease or mortality was found. Relapse of primary disease was significantly associated with mortality (33.3%, n=2, P=0.040), however.
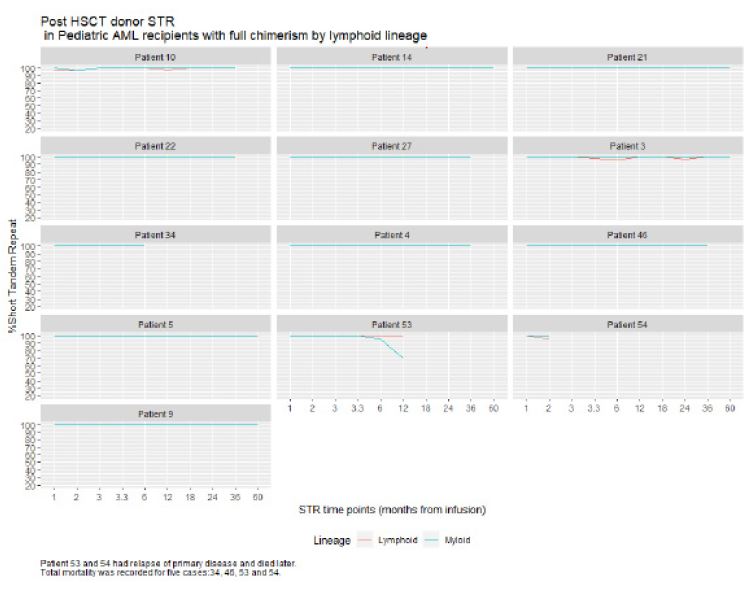
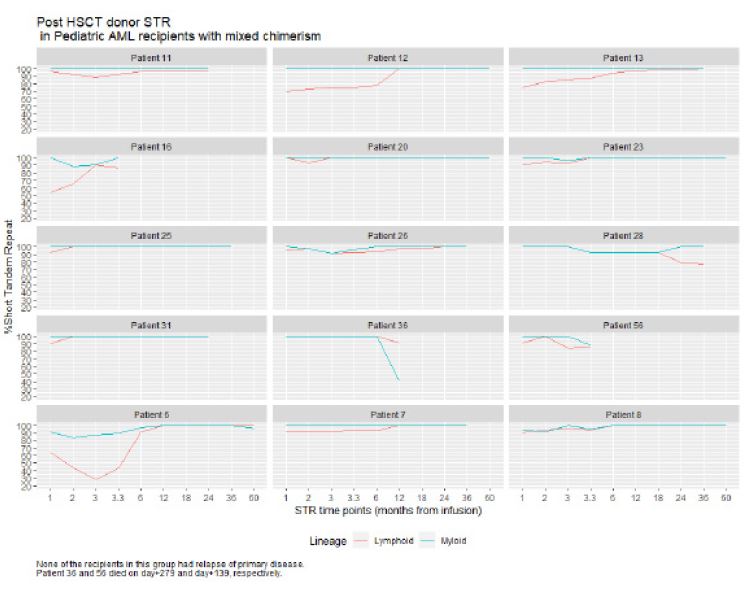
Table 1: Patient characteristics and transplant related parameters by chimerism throughout follow-up.
| Parameters of interest n (%) | FC (13, 46.4%) (<5% Recipient) | MC (15, 53.6%)(≥5% Recipient) | Total (n=28) | P value |
|---|---|---|---|---|
| Gender | 1.000 | |||
| Female | 6 (46.2%) | 8 (53.3%) | 14 (50.0%) | |
| Male | 7 (53.8%) | 7 (46.7%) | 14 (50.0%) | |
| Age at SCT, years,median (range) | 6.4 (0.8-13.0) | 7.5 (0.1-13.7) | 6.9 (0.1– 13.7) | 0.717 |
| Recipient weight(kg) at infusion, median (range) | 16.2 (6.3-51.0) | 21.9 (8.4-76.1) | 19.3 (6.3-76.1) | 0.108 |
| Source of Stem Cells | 0.327 | |||
| Bone marrow | 8 (61.5%) | 12 (80.0%) | 20 (71.4%) | |
| PBSC | 1 (7.7%) | None | 1 (3.6%) | |
| Cord blood | 4 (30.8%) | 3 (20.0%) | 7 (25.0%) | |
| TNCDose1, median (range) | ||||
| Bone marrow/ PBSC | 0.6 (0.2-1.5) | 0.3 (0.1-41.01) | 0.34 (0.13-41.0) | 0.041 |
| Cord blood | 0.1 (0.06-0.1) | 0.05 (0.04-0.1) | 0.09 (0.04-0.13) | 0.400 |
| CD342, median(range) | ||||
| Bone marrow/ PBSC | 7.5 (4.3-10.5) | 3.6 (0.9-8.1) | 5.15 (0.85-10.5) | 0.001 |
| Cord blood | 0.29 (0.05-0.5) | 0.12 (0.09-0.3) | 0.15 (0.05-0.54) | 0.629 |
| Conditioning regimen | 0.759 | |||
| Busulfan, Cyclophosphamide | 4 (30.8%) | 9 (60.0%) | 13 (46.4%) | |
| Busulfan, Cyclophosphamide, ATG | 3 (23.1%) | 2 (913.3%) | 5 (17.9%) | |
| Busulfan, Fludarabine, Thiotepa | 2 (15.4%) | 2 (13.3%) | 4 (14.3%) | |
| Busulfan, Cyclophosphamide, VP-16 | 1 (7.7%) | 1 (6.7%) | 2 (7.1%) | |
| Busulfan, Cyclophosphamide, VP-16, ATG | 1 (7.7%) | 1 (6.7%) | 2 (7.1%) | |
| Fludarabine, Cyclophosphamide, TBI | 1 (7.7%) | None | 1 (3.6%) | |
| Fludarabine, TBI | 1 (7.7%) | None | 1 (3.6%) | |
| Donor Gender | 0.460 | |||
| Female | 4 (30.8%) | 7 (46.7%) | 11 (39.3%) | |
| Male | 9 (69.2%) | 8 (53.3%) | 17 (60.7%) | |
| Donor-Recipient gender matching | 0.755 | |||
| Same gender | 9 (69.2%) | 8 (53.3%) | 17 (60.7%) | |
| Female → male | 1 (7.7%) | 3 (20.0%) | 4 (14.3%) | |
| Male →female | 3 (23.1%) | 4 (26.7%) | 7 (25%) | |
| HLAType | 0.126 | |||
| HLA identical siblings/other relatives | 5 (38.5%) | 11 (73.3%) | 16 (57.1%) | |
| Haploidentical family member | 4 (30.8%) | 1 (6.7%) | 5 (17.9%) | |
| Unrelated HLA1- or 2-AGmismatch (CB) | 4 (30.8%) | 3 (20.0%) | 7 (25.0%) | |
| Days to ANC recovery (median, range) | 17 (12-33) | 18 (13-45) | 17.5 (12-45) | 0.363 |
| BM/PBSC | 16 (14-33) | 15 (13-21) | 16 (13-33) | 0.277 |
| CB | 22 (12-25) | 18 (18-45) | 22 (12-45) | 1.000 |
| Days to platelets recovery (median, range) | 35 (17-160) | 38.5 (17-72) | 37 (17-160) | 0.943 |
| BM/PBSC | 27 (17-64) | 33 (17-60) | 29 (17-64) | 0.552 |
| CB | 63.5 (48-160) | 69 (63-72) | 69 (48-160) | 1.000 |
| Engraftment | 11 (84.6%) | 15 (100.0%) | 26 (92.9%) | 0.206 |
| Primary graftfailure | None | None | None | |
| Secondary graft failure/Relapse of primary | 2 (15.4%) | None | 2 (7.1%) | |
| Acute GvHD | 0.410 | |||
| Acute GvHD(-) | 8 (61.5%) | 12 (80.0%) | 20 (71.4%) | |
| Acute GvHD(+) | 5 (38.5%) | 3 (20.0%) | 8 (28.6%) | |
| Mortality rate | 4 (30.8%) | 2 (13.3%) | 6 (21.4%) | 0.372 |
| Cumulative probability of overall survival | 68.4%±13.1% | 86.7%±8.8% | 78.0%±8.0% | 0.361 |
| Cumulative probability of event-free survival | 68.4%±13.1% | 86.7%±8.8% | 78.0%±8.0% | 0.328 |
1, 109 per kg; 2, 106 per kg.
Abbreviations: HSCT: Hematopoietic stem cell transplant; GVL: Graft versus leukemia; HLA: Human Leukocyte Antigens; OS: Overall survival; EFS: Event free survival.
Discussion
Mixed chimerism has been shown to occur more often in younger patients undergoing non-myeloablative transplants for non-malignant disorders [10-12]. These MC states do not necessarily result in graft failure [13]. Here we show that more than half of our patients undergoing myeloablative conditioning for malignant disease still developed MC with mostly Busulfan based regimens. CD34 dose was significantly associated with MC. Majority of our patients with MC had HLA-matched sibling donors. Our patients had lower incidence of acute- GVHD and better OS in the MC group in keeping with published reports [14,15]. The need for predicting disease relapse after HSCT is clinically significant due to the poor prognosis of early relapse. Given the possibility of early interventions such as rapid tapering of immunosuppression medication and/or transfusion of Donor Lymphocyte Infusion (DLI) has highlighted the importance of monitoring for imminent relapse. Since chimerism analysis in general detects persisting or reappearing recipient cells hence its can be used indirectly to identify surviving leukemia blasts &/or surviving host hematopoiesis. Though in some instances persistence or reappearance of recipient cells can simply reflect survival of normal host hematopoietic cells like most institutions we performed PCR based detection of Short Tandem Repeats (STR-PCR) forchimerism analyses on Peripheral Blood (PB) for surveillance of engraftment with lineage specification after HSCT [16]. This has been the gold standard for most transplant centers in the previous decades, but with a lower Level of Detection (LOD) of 1-5% recipient cells [17,18]. New techniques such as real-time PCR, digital droplet CR and Next Generation Sequencing (NGS) have further increased the accuracy and sensitivity of chimerism analysis. While some studies have shown that an increasing MC is associated with a higher incidence of relapse some have not. A major limitation is the lack of definitive cut-off values across studies [7,8,19,20]. In order to identify a trend in MC cut-off values that indicated a higher risk of relapse we looked at donor T cell chimerism that can reflect donor T cell engraftment and hence can indirectly gauge the degree of Graft-Versus-Leukemia (GVL) effect. In our patient cohort MC does not predict a higher risk of relapse as shown by Mountjoy et. al and others [19,21,22]. Unlike the results by Lee et al. that focused on T-cell MC in adult patients at Days-90-120 to be predictive of relapse we showed that MC within 6-months can be seen without overt relapse. On the contrary in ouranalysis of 28 patients undergoing HSCT, the only 2 relapses and mortality seen were amongstthe 13 patients who had maintained Full Chimerism (FC).
Conclusion
In summary, the role of lymphocyte MC in predicting AML relapse after transplantation has been controversial. A limitation of this study was the lack of MRD results in our patients that could have strengthened this analysis. Integration of chimerism data with higher sensitivity along with MRD measurements should be studied prospectively to develop relapse risk models for potential preemptive intervention in transplant patients with AML.
Declarations
Financial disclosure or funding: This work did not receive any financial support in any form from any funding agency.
Conflict of interest: The authors declare no conflicts of interest.
Informed consent: Data of interest collected from the patients’ medical records were secured as governed by the institutional policies on patient confidentiality and privacy. No informed consents were obtained since this was a retrospective study and all data items collected were already documented in medical charts as part of the patient care and disease management documentation.
Author contributions: All authors certify that they have participated sufficiently in the intellectual content and the analysis of data. Each author has reviewed the final version of the manuscript and approves it for publication. Should the editors request the data upon which the work is based, the authors shall produce it.
Institutional review board approval: This study was submitted to the Institutional Review Board of King Faisal Specialist Hospital and Research Center, Riyadh, Saudi Arabia, before initiation and was approved by the Research Advisory Committee through established procedures via Approval Number 2211058.
Ethical compliance with human/animal study: This study was conducted in compliance with the ethical standards of the responsible institution on human subjects as well as with the Helsinki Declaration.
Data availability: The data can be made available upon reasonable request to the corresponding author.
Funding: None.
Conflict of interest: The authors declare no conflicts of interest.
Authors statement: The manuscript has been read and approved by all the authors, that the requirements for authorship have been met, and that each author believes that the manuscript represents honest work.
Grant support: None.
Financial disclosure: All authors verify that they do not have any financial disclosures to declare.
References
- Ward E, DeSantis C, Robbins A, Kohler B, Jemal A. Childhood and adolescent cancer statistics. CA Cancer J Clin. 2014; 64(2): 83-103. doi:10.3322/caac.21219.
- Lee JH, Ju HY, Hyun JK, et al. Treatment outcome and prognostic factors in relapsed pediatric acute myeloid leukemia. Blood Res. 2023; 58(4): 181-186. doi:10.5045/br.2023.2023152.
- Zarnegar-Lumley S, Caldwell KJ, Rubnitz JE. Relapsed acute myeloid leukemia in children and adolescents: current treatment options and future strategies. Leukemia. 2022; 36(8): 1951-1960. doi:10.1038/s41375-022-01619-9.
- Moritake H, Tanaka S, Miyamura T, et al. The outcomes of relapsed acute myeloid leukemia in children: Results from the Japanese Pediatric Leukemia/Lymphoma Study Group AML-05R study. pediatr Blood Cancer. 2021; 68(1): e28736. doi:10.1002/pbc.28736.
- Sharma A, Li Y, Huang S, et al. Outcomes of pediatric patients who relapse after first HCT for acute leukemia or MDS. Bone Marrow Transplant. 2021; 56(8): 1866-1875. doi:10.1038/s41409-021-01267-0.
- Bejanyan N, Weisdorf DJ, Logan BR, et al. Survival of patients with acute myeloid leukemia relapsing after allogeneic hematopoietic cell transplantation: A center for international blood and marrow transplant research study. Biol Blood Marrow. Transplant. 2015; 21(3): 454-459. doi:10.1016/j.bbmt.2014.11.007.
- Rettinger E, Willasch AM, Kreyenberg H, et al. Preemptive immunotherapy in childhood acute myeloid leukemia for patients showing evidence of mixed chimerism after allogeneic stem cell transplantation. Blood. 2011; 118(20): 5681-5688. doi: 10.1182/blood-2011-04-348805.
- Qin XY, Li GX, Qin YZ, et al. Quantitative chimerism: An independent acute leukemia prognosis indicator following allogeneic hematopoietic SCT. Bone Marrow Transplant. 2014; 49(10): 1269-1277. doi:10.1038/bmt.2014.158.
- Cousin E, Oger E, Dalle JH, et al. Assessment of chimerism and immunomodulation to prevent post-transplantation relapse in childhood acute myeloblastic leukemia: is it the right approach?. Pediatr Hematol Oncol. 2020; 37(3): 259-268. doi:10.1080/08880018.2020.1717697.
- Hamidieh AA, Behfar M, Pourpak Z, et al. Long-term outcomes of fludarabine, melphalan and antithymocyte globulin as reduced-intensity conditioning regimen for allogeneic hematopoietic stem cell transplantation in children with primary immunodeficiency disorders: A prospective single center study. Bone Marrow Transplant. 2016; 51(2): 219-226. doi:10.1038/bmt.2015.277.
- Satwani P, Cooper N, Rao K, Veys P, Amrolia P. Reduced intensity conditioning and allogeneic stem cell transplantation in childhood malignant and nonmalignant diseases. Bone Marrow Transplant. 2008; 41(2): 173-182. doi:10.1038/sj.bmt.1705923.
- Faraci M, Bagnasco F, Leoni M, et al. Evaluation of Chimerism Dynamics after Allogeneic Hematopoietic Stem Cell Transplantation in Children with Nonmalignant Diseases. Biol Blood Marrow Transplant. 2018; 24(5): 1088-1093. doi:10.1016/j.bbmt.2017.12.801.
- Llaurador G, Nicoletti E, Prockop SE, et al. Donor-Host Lineage-Specific Chimerism Monitoring and Analysis in Pediatric Patients Following Allogeneic Stem Cell Transplantation: Influence of Pretransplantation Variables and Correlation with Post-Transplantation Outcomes. Transplant Cell Ther. 2021; 27(9): 780.e1-780.e14. doi:10.1016/j.jtct.2021.05.02.
- Alimoghaddam K, Ghaffari H, Foroughi F, et al. Effects of chimerism on graft-versus-host disease, disease recurrence, and survival after HLA-identical marrow transplantation in Iran. Arch Iran Med. 2006; 9(2): 99-103.
- Sheth V, Potter V, De Lavallade H, et al. Mixed T cell lineage chimerism in acute leukemia/MDS using pre-emptive donor lymphocyte infusion strategy-Is it prognostic?-a single-center retrospective study. Blood Cancer J. 2021; 11(7): 128. doi:10.1038/s41408-021-00519-y.
- Khan S, AlSaif Z, Siddiqui K, et al. Is Mixed Chimerism Post-allogeneic Hematopoietic Stem Cell Transplantation in Pediatric Acute Lymphoid Leukemia a Prognostic Factor for Relapse?. Hematol Oncol Stem Cell Ther. 2023; 17(1): 72-78. doi:10.56875/2589-0646.1112.
- Lion T, Daxberger H, Dubovsky J, et al. Analysis of chimerism within specific leukocyte subsets for detection of residual or recurrent leukemia in pediatric patients after allogeneic stem cell transplantation. Leukemia. 2001; 15(2): 307-310. doi:10.1038/sj.leu.2402017.
- Clark JR, Scott SD, Jack AL, et al. Monitoring of chimerism following allogeneic haematopoietic stem cell transplantation (HSCT): technical recommendations for the use of Short Tandem Repeat (STR) based techniques, on behalf of the United Kingdom National External Quality Assessment Service for Leucocyte Immunophenotyping Chimerism Working Group. Br J Haematol. 2015; 168(1): 26-37. doi:10.1111/bjh.13073.
- Haugaard AK, Kofoed J, Masmas TN, et al. Is microchimerism a sign of imminent disease recurrence after allogeneic hematopoietic stem cell transplantation? A systematic review of the literature. Blood Rev. 2020; 44: 100673. doi:10.1016/j.blre.2020.100673.
- Koldehoff M, Steckel NK, Hlinka M, Beelen DW, Elmaagacli AH. Quantitative analysis of chimerism after allogeneic stem cell transplantation by real-time polymerase chain reaction with single nucleotide polymorphisms, standard tandem repeats, and Y-chromosome-specific sequences. Am J Hematol. 2006; 81(10): 735-746. doi:10.1002/ajh.20693.
- Huisman C, De Weger RA, De Vries L, Tilanus MG, Verdonck LF. Chimerism analysis within 6 months of allogeneic stem cell transplantation predicts relapse in acute myeloid leukemia. Bone Marrow Transplant. 2007; 39(5): 285-291. doi:10.1038/sj.bmt.1705582.
- Mountjoy L, Palmer J, Kunze KL, et al. Does early chimerism testing predict outcomes after allogeneic hematopoietic stem cell transplantation?. Leuk Lymphoma. 2021; 62(1): 252-254. doi:10.1080/10428194.2020.1827249.