SciBase Journals
SciBase Addiction & Recovery
- Article Type: Research Article
- Volume 1, Issue 1
- Received: Jul 04, 2024
- Accepted: Aug 28, 2024
- Published Online: Sep 04, 2024
Exploring the Influence of BMI on Gait Metrics: A Comprehensive Analysis of Spatiotemporal Parameters and Stability Indicators
Lianne Koinis1,4-6; Monish Maharaj1-4; Pragadesh Natarajan1-4; R Dineth Fonseka1-4; Vinuja Fernando3-4; Ralph J Mobbs1-4*
1Neuro Spine Surgery Research Group (NSURG), Randwick, Australia.
2Neuro Spine Clinic, Prince of Wales Private Hospital, Randwick, Australia.
3Faculty of Medicine, University of New South Wales (UNSW), Randwick, Australia.
4Wearable and Gait Assessment Research Group (WAGAR), Prince of Wales Private Hospital, Randwick, Australia.
5Faculty of Psychology, University of New South Wales (UNSW), Sydney, Australia.
6Faculty of Psychology, Monash University, Sydney, Australia.
*Corresponding Author: Ralph J Mobbs
Neuro Spine Surgery Research Group (NSURG), Randwick,
Australia.
Email: almeidacarvalho.manager@wagar.au
Abstract
Background: Gait analysis is a vital tool for evaluating overall health and predicting outcomes such as mortality and cognitive decline. This study explores how normal and obese BMI categories differently impact gait dynamics, addressing gaps in understanding body composition’s effect on specific gait parameters.
Research question: The primary objective is to investigate the variances in spatiotemporal gait parameters-specifically, gait speed, step length, cadence, and double support time—between normal and obese BMI groups, to understand the effects of obesity on gait.
Methods: This observational case-control study analyzed spatiotemporal gait metrics from 163 participants, using Inertial Measurement Units (IMUs) to collect data on various gait parameters. Statistical analyses explored the relationship between BMI categories and these metrics.
Results: No significant differences were found in gait speed, cadence, stride duration, or double support time between the normal and obese groups. However, significant differences were identified in age, hypertension prevalence, balance problems, and the incidence of falls, emphasizing the complex effects of obesity on factors influencing gait stability.
Significance: The study contributes to our understanding of obesity’s impact on gait by highlighting the need to consider associated health and stability parameters. These findings prompt a re-evaluation of how BMI is integrated into clinical gait assessments and emphasize the necessity for personalized healthcare strategies. Our research highlights the importance of future studies with larger, more diverse populations and a wider array of biomechanical measures to dissect the relationship between BMI, body composition, and gait dynamics.
Keywords: BMI; Gait dynamics; Spatiotemporal gait parameters; Mobility; Inertial Measurement Units (IMUs); Body composition analysis.
Citation: Koinis L, Maharaj M, Natarajan P, Fonseka RD, Mobbs RJ, et al. Exploring the Influence of BMI on Gait Metrics: A Comprehensive Analysis of Spatiotemporal Parameters and Stability Indicators. SciBase J Addict Recovery. 2024; 1(1): 1001.
Introduction
Gait pattern, an objective indicator of physical health, correlates with critical health outcomes including mortality and cognitive decline [1]. It serves as a prognostic tool for predicting functional dependency, frailty, and overall well-being [2]. This study explores how body composition affects gait dynamics by comparing normal and obese BMI categories, focusing on gaitspeed, step length, cadence, and double support time. Given BMI’s influence on biomechanical functions and its association with mobility issues and diseases, we aim to investigate the effects of obesity on gait, noting that people with obesity may experience up to a 15% reduction in gait speed and a 25% decrease in step length compared to those with a normal BMI [3]. Through this analysis, we aim to uncover specific gait alterations linked to obesity and highlight potential direct healthcare intervention targets that respect these findings, such as personalized physical therapy and targeted exercise programs. As described by Fonseka RD et al. (2023), utilizing a single-point wearable sensor to assess lumbar spine patients pre- and postoperatively highlighted the utility of gait metrics in evaluating surgical outcomes and rehabilitation progress [4].
Obesity may impact gait dynamics by inducing central resistance to hormones like leptin and insulin that may decrease energy expenditure and alter neuroendocrine connections essential for gait coordination [5]. Moreover, the alteration in body weight distribution and biomechanics due to increased adipose tissue in obesity leads to changes in walking patterns and overall movement efficiency [6]. These factors contribute to a notable decrease in step length (5-10 cm) and cadence (up to 10 steps/min) in people with obesity, suggesting either energy-conservation tactics or fitness-related limitations in ability as the main drivers. Additionally, the extension of double support time by up to 2% during the gait cycle among people with obesity hints at adaptations for added stability [3].
BMI serves as an indirect measure of health, classifying individuals into normal (BMI 18.5 to 24.9) and obese (BMI≥30) categories to assess body fat and health risks [7]. Mobbs (2020) has highlighted that obesity alters gait dynamics, leading to significant modifications like reduced step count in comparison to those of normal BMI [8]. These changes emphasize the need for health strategies that address BMI differences, aiming to improve health outcomes and quality of life by addressing obesity’s impact on mobility and chronic disease risks.
Although there are large volume references for cardiovascular health metrics across BMI categories [9], to our knowledge, a cohesive large-scale database correlating BMI with distinct gait patterns is not published. Our study seeks to establish a normative gait metric database for normal and obese BMI categories, offering healthcare practitioners valuable insights to assess and tackle mobility issues with BMI-adapted approaches. By mapping body composition against gait dynamics, our research aims to refine clinical evaluations and facilitate targeted health interventions that significantly enhance life quality, drawing from literature that documents observable gait differences across BMI groups [8,2].
Literature review: Research has shown that BMI influences gait dynamics in various ways. Browning and Kram (2007) demonstrated that obese individuals exhibit increased energy expenditure during walking due to altered biomechanics, leading to reduced gait efficiency [10]. Noted that children with obesity have different gait patterns, characterized by wider steps and lower gait speed, to maintain balance and stability [11]. Additionally, found that weight loss in obese patients led to significant improvements in gait parameters, emphasizing the impact of body composition on mobility [12]. These studies highlight the importance of understanding how BMI affects gait to develop effective interventions for improving mobility in obese individuals.
Subjects
The study’s cohort initially consisted of 320 normative subjects. Exclusion criteria included: < 18 years of age, non-binary gender identification, an inability to walk at least 50 meters independently, were not within either normal or obese BMI categories, pregnancy, or any medical conditions known to alter gait patterns, such as stroke, lumbar spinal stenosis, multiple sclerosis, or significant degenerative and/or rheumatological conditions affecting the hip, knee, and spine, a total of 214 participants were included in the analysis for health-related and motion metrics variables.
Of the 320 patients recruited for the study, 163 remained following the application of exclusion criteria, representing 126 individuals with a normal BMI and 37 with an obese BMI.
Material and methods
Ethics
Approval was obtained from the South-Eastern Sydney Local Health District, New South Wales, Australia (HREC 17/184). All participants provided written informed consent.
Data collection
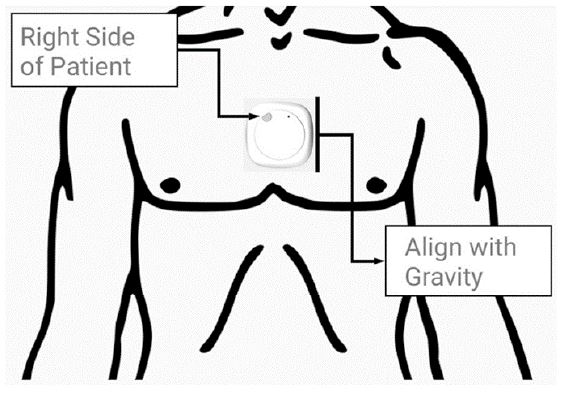
Following the acquisition of informed consent, participants underwent a structured interview to gather comprehensive demographic data including age, weight, height, BMI, smoking status and the presence of either hypertension or diabetes. The MetaMotionC Inertial Measurement Unit (IMU) by Mbientlab Inc (California, USA), equipped with a 16-bit triaxial accelerometer (100Hz), gyroscope (100Hz), and magnetometer (0.3μT at 25Hz) was used to derive gait data. This sensor was placed at the sternal angle of each participant to ensure optimal data capture (Figure 1). After a brief calibration period to ensure the IMU’s correct orientation, participants were instructed to walk a 50-meter distance along a flat, unobstructed concrete pathway. This walk was performed unobserved to simulate natural walking conditions and pace.
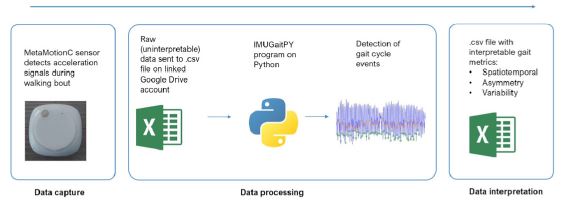
Data capture was facilitated through a Bluetooth™ connection to an Android™ smartphone running the custom developed IMU Gait Recorder application. The raw data collected was then processed using IMUGaitPY, a custom coded Python package by the WAGAR Group (Sydney, Australia) for gait metric analysis. This software was instrumental in extracting the relevant spatiotemporal metrics from the collected data, with further methodological details provided in Figure 2. Metrics collected included stride duration, cadence, double support time, gait speed and daily step count.
AI algorithm details: The AI algorithm utilized in IMUGaitPY involves a multi-layered approach combining data preprocessing, feature extraction, and machine learning classification. The raw data undergoes noise filtering and segmentation to isolate individual gait cycles. Feature extraction focuses on key spatiotemporal metrics, including stride duration, cadence, and double support time. These features are then analyzed using machine learning models such as Random Forest and Support Vector Machines (SVM) to classify gait patterns and predict deviations based on BMI categories. The algorithm’s performance is validated through cross-validation and evaluated using metrics such as accuracy, precision, and recall.
Data analysis
This observational case-control study focuses on 163 participants across normal and obese BMI categories, aiming to analyse spatiotemporal gait metrics and establish variances in gait parameters between the two groups. BMI was collected as a categorical variable and correlated with IMU derived gait metrics.
Inferential and descriptive analysis of data was carried out (Table 1). The distribution normality of our dataset was assessed via Shapiro-Wilk and Kolmogorov-Smirnov tests. For normally distributed variables, we computed descriptive statistics, including means and standard deviations, to summarize central tendency and variability. Non-parametric tests (Mann-Whitney-U) were performed for non-normal data with medians and Interquartile Ranges (IQRs) reported to present central tendency and variability. Associations among categorical variables were examined using the Chi-square test, while Pearson’s correlation coefficient facilitated the exploration of relationships between gait metrics and BMI categories. Statistical significance was established at a p-value< 0.05. All statistical analysis was executed using IBM SPSS software version 27.0 (Armonk, NY).
Results
Basic descriptive statistics are presented in Table 1. The analysis revealed statistically significant differences in age, hypertension, problems with balance, and the incidence of falls between the normal and obese groups. Specifically, the obese group had a higher average age compared to the normal group (p< 0.01*). However, there was no statistically significant difference in height between the groups (p=0.90824).
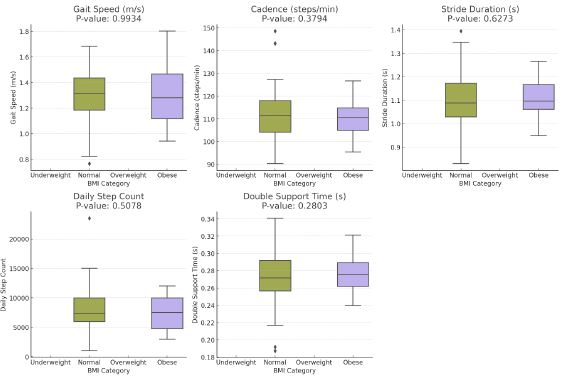
In evaluating gait metrics, including stride duration, cadence, gait speed, daily step count, and double support time, there were no significant differences between the normal and obese BMI categories (all p-values>0.05).
The results revealed a significant difference in hypertension prevalence between BMI categories, with the obese group exhibiting a higher percentage (21.62% vs. 6.35%, p=0.003).
Furthermore, the incidence of falls in the last 12 months was significantly higher among people with obesity than their normal-weight counterparts (11.43% vs. 0.80%, p=0.015). A higher percentage of people with obesity reported balance problems (13.51% vs. 4.00%, p=0.048).
Table 1: Demographic characteristics of study participants.
| Demographic | Normal (n=126) | Obese (n=37) | p-Value |
|---|---|---|---|
| Age (years) | 36.0±11.33 | 44.4±12.52 | 0.00065** |
| Height (cm) | 170±9.97 | 155±11.24 | 0.90824 |
| Sex (% male) | 44.44% | 59.46% | - |
| Smoking (% of yes) | 13.49% | 21.62% | 0.212 |
| Diabetes (% of yes) | 3.97% | 2.70% | 0.762 |
| Hypertension (% of yes) | 6.35% | 21.62% | 0.003** |
| Problems with balance? (% of yes) | 4.00% | 13.51% | 0.048** |
| Falls in last 12 months? (% of yes) | 0.80% | 11.43% | 0.015** |
Table 2: Continuous metrics averages by BMI category.
| Metric/Category | Normal | Obese | P-values |
|---|---|---|---|
| Stride Duration (seconds) | 1.101 | 1.108 | 0.627 |
| Cadence (steps/min) | 111.23 | 109.90 | 0.379 |
| Gait Speed (m/s) | 1.31 | 1.24 | 0.993 |
| Daily Step Count (steps) | 7745.97 | 7331.37 | 0.508 |
| Double Support Time (s) | 0.26 | 0.27 | 0.280 |
Discussion
The objective of this prospective observational cohort study was to establish a comprehensive normative database for spatiotemporal gait metrics across different BMI categories, with the intent of serving as a reference for detecting anomalies in gait patterns.
Our findings, revealing no significant differences in cadence, gait speed, stride duration, daily step count, or double support time between Normal and Obese BMI categories, diverge from existing literature that reported variations in gait dynamics with BMI differences [13]. For instance, in a study by involving 2809 participants, it was demonstrated that increasing BMI is associated with decreased gait speed, and obesity significantly raises the likelihood of falls and related injuries [14]. This investigation into real-world gait speed in relation to frailty and handgrip strength revealed that gait speed metrics significantly improved frailty detection and handgrip strength prediction, highlighting a profound link between BMI, gait dynamics, and physical function [15].
Our results identified a correlation between BMI and factors influencing stability, specifically balance and fall risk, suggesting that while excess weight may contribute to declines in functional stability, it may not uniformly affect basic gait metrics. This observation suggests that the effect of obesity on physical function, especially in older adults, might be influenced by factors beyond BMI [15]. For example, the age differences observed within our BMI may have confounded our data, although one would generally suspect those of older age to exhibit a broader and more diminished range of gait metrics, which was not directly observed. This complexity is further magnified by not directly accounting for muscle strength and physical activity levels in our analysis, despite their acknowledged influence on gait dynamics [15]. Although we previously sought to integrate these multifactorial aspects through the subjective and objective quality of life score (SOQOL™) (2023), it does not directly address the impact of BMI [16].
To further explore the impact of age on gait characteristics, our findings indicate age significantly influences gait metrics analysis across BMI categories. The obese population group was older on average than the normal group (p<0.01*), emphasizing age’s critical role in gait evaluation. This highlights the importance of age-specific cutoffs in analyzing gait dynamics for a clearer understanding of how age and BMI interact with gait. Incorporating age-focused analysis could enrich our results, offering objective insights and aligning our study with existing literature on the complex interplay between age, BMI, and gait dynamics [17].
The increase in fall incidents and balance problems, coupled with a higher prevalence of hypertension in the obese population group, emphasize the complex consequences of obesity on gait and stability. This complexity is highlighted by Natarajan P et al.’s review on gait and mobility metric capture postoperatively [18] and Koinis et al.’s exploration of smartphones and wearable devices in mental health monitoring [19]. These studies broaden gait analysis applications, suggesting its utility in mental health status indication, thus advocating for expansive studies that encompass the interplay of age, body composition, and physical activity in gait and stability analysis.
Strengths, limitations, and future directions
This research provides a data-driven insight into BMI’s popotential effects on gait metrics, enhancing the understanding of the body mass-gait mechanics relationship, particularly through the lens of BMI-associated age, balance, and fall risk. Our examination of gait metrics across BMI categories delivers essential data for clinicians and researchers, contributing to the ongoing exploration on BMI’s influence on gait despite no direct correlation in observed spatiotemporal parameters.
However, the study’s limited sample size might have restricted our ability to detect significant differences, which is a concern considering the observed disparities in age and balance measures, hinting at adiposity-related stability impacts. This highlights the need for larger, more diverse, as emphasized by, who stressed the importance of inclusivity in research samples [20].
Future research may build on our findings by incorporating detailed body composition analyses and a broader range of biomechanical measures, including those that directly assess stability and balance. Additional measures, like stride length, step width, energy expenditure, and joint kinetics, may clarify the biomechanical impact of obesity on gait and stability, as also suggested by the work of. Such research should consider the implications of age and how age-related changes in body composition may interact with BMI to affect gait dynamics [21].
Although this study did not find significant differences in basic gait metrics, the observed relationships with age, balance, and falls reinforce the multifaceted nature of the effects of obesity on mobility. This study sets a foundation for future inquiries to refine our understanding of gait mechanics in the context of BMI, with the goal of enhancing gait analysis methodologies and clinical interventions for mobility-related conditions.
Conclusion
This study found no significant impact of BMI on gait metrics but identified obesity as a factor associated with age-related health issues, balance problems, and a higher incidence of falls. These insights challenge the presumed relationship between BMI and gait, emphasizing the need for more in-depth research to unravel the complex factors influencing mobility.
Declarations
Acknowledgments: The NeuroSpine Surgery Research Group (NSURG) aided with manuscript production. The NeuroSpineClinic, Sydney Australia, provided clinic assistance for authors.
Funding: None.
Conflicts of interest: RJM & all authors are members of the Wearables of Gait Assessment Research (WAGAR) Group, Sydney, Australia. None of the authors have any conflicts to declare with regards to this article.
Ethical statement: The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ethics approval: Ethics approval was obtained from the South-eastern Sydney Local Health District (HREC 17/184). All Patient provided written, informed consent for the procedure and access to data on their ongoing clinical evaluation and radiological outcomes.
Open access statement: This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial-NoDerivs 4.0 International License (CC BY-NC-ND 4.0), which permits the non-commercial replication and distribution of the article with the strict proviso that no changes or edits are made and the original work is properly cited (including links to both the formal publication through the relevant DOI and the license). See: https://creativecommons.org/licenses/by-nc-nd/4.0/.
References
- De la Cámara MÁ, Higueras-Fresnillo S, Sadarangani KP, Esteban-Cornejo I, Martinez-Gomez D, et al. Clinical and Ambulatory Gait Speed in Older Adults: Associations with Several Physical, Mental, and Cognitive Health Outcomes. Phys Ther. 2020; 100(4): 718-727. doi:10.1093/ptj/pzz186.
- Andreasen J, Aadahl M, Sørensen EE, Eriksen HH, Lund H, et al. Associations and predictions of readmission or death in acutely admitted older medical patients using self-reported frailty and functional measures. A Danish cohort study. Arch Gerontol Geriatr. 2018; 76: 65-72. doi:10.1016/j.archger.2018.01.013.
- Wong-On M, Murillo-Cuzza G. Fundamentos fisiopatológicos de la obesidad y su relación con el ejercicio. Acta Médica Costarricense. 2004; 46(Suppl 1): 15-24. http://www.scielo.sa.cr/scielo.php?script=sci_arttext&pid=S0001-60022004000500005&lng=en&tlng=.
- Fonseka RD, Natarajan P, Maharaj MM, Koinis L, Sy L, et al. Objective Gait Analysis Using a Single-Point Wearable Sensor to Assess Lumbar Spine Patients Pre- and Postoperatively. Surgical Techniques Development. 2024; 13(1): 58-75. doi:10.3390/std13010004.
- Kyrou I, Randeva HS, Tsigos C, et al. Clinical Problems Caused by Obesity. In: Feingold KR, Anawalt B, Blackman MR, et al. Editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc. 2000. https://www.ncbi.nlm.nih.gov/books/NBK278973/
- Malatesta D, Favre J, Ulrich B, et al. Effect of very large body mass loss on energetics, mechanics and efficiency of walking in adults with obesity: Mass-driven versus behavioural adaptations. J Physiol. 2022; 600(4): 979-996. doi:10.1113/JP281710.
- Nuttall FQ. Body Mass Index: Obesity, BMI, and Health: A Critical Review. Nutr Today. 2015; 50(3): 117-128. doi:10.1097/NT.0000000000000092.
- Mobbs RJ. Gait velocity (walking speed) is an indicator of spine health, and objective measure of pre and post intervention recovery for spine care providers. J Spine Surg. 2020; 6(2): 353-355. doi:10.21037/jss-20-602.
- Ghazizadeh H, Mirinezhad SMR, Asadi Z, et al. Association between obesity categories with cardiovascular disease and its related risk factors in the MASHAD cohort study population. J Clin Lab Anal. 2020; 34(5): e23160. doi:10.1002/jcla.23160.
- Browning RC, Kram R. Effects of obesity on the biomechanics of walking at different speeds. Med Sci Sports Exerc. 2007; 39(9): 1632-1641. doi:10.1249/mss.0b013e318076b54b.
- Hills AP, Parker AW, Byrne NM. Estimated energy expenditure in overweight and obese adults. Int J Obes Relat Metab Disord. 2002; 26(6): 707-709. doi:10.1038/sj.ijo.0801976.
- Sartorio A, Lafortuna CL, Conte G, Faglia G, Narici MV. Changes in motor control and muscle performance after a short-term body mass reduction program in obese subjects. J Endocrinol Invest. 2001; 24(6): 393-398. doi:10.1007/BF03343891.
- Natarajan P, Fonseka RD, Kim S, Betteridge C, Maharaj M, et al. Analysing gait patterns in degenerative lumbar spine diseases: A literature review. J Spine Surg. 2022; 8(1): 139-148. doi:10.21037/jss-21-91.
- Abualait T, Ahsan M. Comparison of gender, age, and body mass index for spatiotemporal parameters of bilateral gait pattern. F1000Res. 2021; 10: 266. doi:10.12688/f1000research.51700.2.
- Oltani A, Abolhassani N, Marques-Vidal P, et al. Real-world gait speed estimation, frailty and handgrip strength: A cohort-based study. Sci Rep. 2021; 11: 18966. https://doi.org/10.1038/s41598-021-98359-0.
- Gonzalez M, Gates DH, Rosenblatt NJ. The impact of obesity on gait stability in older adults. J Biomech. 2020; 100: 109585. doi:10.1016/j.jbiomech.2019.109585.
- Mobbs RJ, Fonseka RD, Natarajan P, Koinis L, Maharaj M. The Subjective and Objective Quality of Life Score (SOQOLTM) for the Quantification of General Health Status: A Preliminary Study with Initial Normative Population Values. J Patient Rep Outcomes. 2024; 8(1): 7. doi:10.1186/s41687-024-00684-1.
- Natarajan P, Fonseka RD, Maharaj MM, Koinis L, Mobbs RJ. Continuous Data Capture of Gait and Mobility Metrics Using Wearable Devices for Postoperative Monitoring in Common Elective Orthopaedic Procedures of the Hip, Knee, and Spine: A Scoping Review. J Orthop Surg Res. 2023; 18(1): 812. doi:10.1186/s13018-023-04303-5.
- Koinis L, Mobbs RJ, Fonseka RD, Natarajan P. A Commentary on the Potential of Smartphones and Other Wearable Devices to Be Used in the Identification and Monitoring of Mental Illness. Ann Transl Med. 2022; 10(24): 1420. doi:10.21037/atm-21-6016.
- Lee SS, Fullerton SM, McMahon CE, et al. Targeting Representation: Interpreting Calls for Diversity in Precision Medicine Research. Yale J Biol Med. 2022; 95(3): 317-326.
- Nantel J, Mathieu ME, Prince F. Physical activity and obesity: Biomechanical and physiological key concepts. J Obes. 2011; 2011: 650230. doi:10.1155/2011/650230.